Table of Contents
Unit 2. 12
Human Body. 12
Sub-unit 2.1. 13
The Cardiovascular System.. 13
Learning objectives: 14
Lesson 1: Anatomy of the cardiovascular system.. 14
Heart 14
Activity 14
Activity 15
Activity 17
Coverings of the heart and their functions. 17
Layers of the heart wall 17
Chambers (rooms) of the heart 17
Heart valves. 17
Blood vessels. 20
Arteries 20
Veins 20
Capillaries 20
Activity 20
Coronary circulation. 21
Blood. 22
Lesson 2: Physiology of the cardiovascular system.. 24
Pathway of blood through the heart 24
Left side of the heart 24
Right side of the heart 24
Activity 25
Activity 26
Lesson 3: Practical 27
Vital health signs: pulse and blood pressure. 27
Pulse or heart rate. 27
Activity 27
Blood pressure. 29
Activity 29
Types of blood pressure apparatus. 29
Activity 32
Learn to take blood pressure. 32
Lesson 4: Disease states. 34
Atherosclerosis. 34
Activity 35
Angina pectoris. 35
Myocardial infarction (heart attack) 35
Hypertension. 37
Class room evaluation. 38
Sub-unit 2.2. 53
The Gastrointestinal System.. 53
Learning objectives: 77
Introduction. 77
Lesson 1: Anatomy of the digestive system.. 77
Gastrointestinal tract: 77
Lower gastrointestinal tract 78
Activity 83
Lesson 2: Physiology of the digestive system.. 87
Digestion. 87
Digestion in the mouth. 87
Digestion in the stomach. 87
Digestion in the small intestine. 87
Digestion in the large intestine. 88
Role of liver and pancreas in digestion. 88
Activity 88
Lesson 3: Disease states. 89
Waterborne diseases. 89
Activity 89
Transmission. 89
Causes of Waterborne Diseases. 89
Food-borne diseases. 91
Activity 91
Dehydration. 92
Treatment Mild dehydration. 94
WHO (2004) recipe for home-made ORS. 95
Ten things you should tell the caregiver who is rehydrating a child. 95
Malnutrition. 96
Types of Malnutrition. 96
Causes of malnutrition. 96
Lesson 4: Practical 97
Activity 97
Role play 97
Class room evaluation. 98
Sub-unit 2.3. 77
Pulmonary System.. 77
Learning objectives: 103
Lesson 1: Anatomy of the System.. 103
Activity. 110
Lesson 2: Physiology of the respiratory system.. 111
Respiration. 111
Lesson 3: Disease states. 115
Pneumonia. 115
Causes 115
How does pneumonia occur?. 115
Common signs and symptoms. 116
Other symptoms. 116
Diagnosis 116
Prevention of pneumonia. 118
Pulmonary Tuberculosis. 119
Facts about tuberculosis. 119
Local symptoms of pulmonary TB. 120
Systemic symptoms of pulmonary TB. 120
Examinations and Tests. 120
Treatment 120
Prevention 121
Important things about tuberculosis to tell patients. 121
Acute Respiratory Infections. 123
Upper Respiratory Tract 123
Lower Respiratory Tract 123
Lesson 4: Practical 124
Measurement and recording of respiratory rate. 124
Average respiratory rates, by age. 125
Causes of increased respiratory rate. 125
Causes of decreased respiratory rate. 125
Class room evaluation. 126
Sub-unit 2.4. 103
The Musculoskeletal System & Skin. 103
Learning objectives: 139
Introduction. 139
Lesson 1: Anatomy of the Musculoskeletal System.. 139
Bones. 139
Types of bones. 144
Major long bones of the limbs. 145
Upper limb 145
Lower limb 145
Muscles. 146
Activity 148
Joints. 150
Lesson 2: Physiology of the Musculoskeletal System.. 151
Bones. 151
Activity 151
Muscles. 151
Activity 152
Joints. 152
Activity 152
Activity 154
Lesson 3: Disease states. 155
Fractures. 155
Activity 156
Different types of fractures. 156
First Aid Management. 158
How can the risk for fractures be minimised?. 159
Lesson 4: Practical 162
Activity 162
Activity 163
Lesson 5: Skin. 168
Anatomy. 168
Functions of Skin. 170
Common Skin Disorders. 171
Rashes 171
Viral infections: 171
Bacterial infections: 171
Fungal infections: 172
Parasitic infections: 172
Scabies 172
Pigmentation disorders: 177
Class room evaluation. 179
Sub-unit 2.5. 185
The Nervous System.. 185
Learning objectives: 171
Lesson 1: Anatomy of the Nervous System.. 171
Division of the Nervous System.. 171
The Central Nervous System (CNS) 174
Brain 174
Activity 175
Activity: 176
Spinal Cord 179
The peripheral nervous system (PNS) 180
Sensory-somatic nervous system.. 180
Autonomic Nervous System (ANS): 184
Sympathetic nervous system.. 184
Parasympathetic nervous system.. 185
Activity 185
Lesson 2: Physiology of the nervous system.. 188
Lesson 3: Disease states. 189
Head Injury. 189
Definition 189
Causes 189
Signs and symptoms. 189
Long-term effects of head injury. 191
Diagnostic aids. 191
First Aid 192
Management of mild head injury. 192
Management of moderate to severe head injury. 193
Prevention 194
Lesson 4: Practical 195
Lesson 5: Spinal cord injury: 196
First aid. 196
Signs 196
First Aid Treatment: 197
Lesson 6: Stroke. 198
Signs of a stroke. 198
What to do if stroke is suspected?. 198
Follow the DRABC Action Plan. 198
Class room evaluation. 201
Sub-unit 2.6. 206
The Excretory System.. 206
Learning objectives: 207
Introduction. 207
Lesson 1: Anatomy of the Urinary System.. 207
Kidneys. 207
Urinary bladder. 208
Ureters. 208
Urethra. 208
Activity 211
Figure 5: Location of kidneys in the body (back of the body) 211
Figure 6: Location of kidneys, ureters and bladder in the body (front of the body) 211
Lesson 2: Physiology of the urinary system.. 213
Activity 213
Activity 214
Lesson 3: Disease states. 215
Presence of protein in urine. 215
Diabetic Nephropathy. 215
High Blood Pressure. 216
Acute Renal Failure. 216
Chronic Kidney Disease. 216
End-Stage Renal Disease. 216
Urinary incontinence. 216
Infections. 216
Urethritis. 218
Catheterisation. 218
Long term (indwelling) urethral catheters. 218
Short-term catheterisation. 219
Lesson 4: Practical 220
Identify the various types of catheters. 220
Insertion of a catheter (men) 223
Insertion of a catheter (women) 223
Insertion of a Straight catheter. 224
Insertion of a Foley catheter. 224
Activity 227
Things you should tell the patient with an inserted catheter. 227
How to remove a catheter. 228
Class room evaluation. 229
Sub-unit 2.7. 234
Reproductive System.. 234
Learning objectives: 235
1. Lesson 1: Anatomy of the reproductive system.. 235
Male reproductive system.. 235
Female reproductive system.. 237
Lesson 2: Physiology of the male and female reproductive systems. 242
Males. 242
Females. 242
Puberty. 243
Menopause. 243
Class room evaluation. 245
Sub-unit 2.8. 250
The Endocrine System.. 250
Learning objectives: 251
Introduction. 251
1. Lesson 1: Anatomy of the endocrine system.. 251
Exocrine glands. 251
Endocrine glands. 251
Activity 254
Lesson 2: Physiology of the endocrine system.. 255
Hormones. 255
Activity 256
Hypothalamus. 256
Pituitary gland. 257
Anterior pituitary lobe. 257
Posterior pituitary lobe. 258
Pineal Gland. 258
Thyroid gland. 259
Parathyroid gland. 259
Increases blood calcium levels. 259
Thymus gland. 259
Pancreas. 260
Adrenal glands. 260
Adrenal cortex. 260
Adrenal medulla. 260
Activity. 261
Disease states. 262
Thyroid hormones. 262
Insulin. 262
Activity 263
Class room evaluation. 268
Notes. 271
Unit 2
Human Body
Sub-unit 2.1
The Cardiovascular System
Learning objectives:
After completing sub-unit 2.1, students will be able to:
a. demonstrate how to mark location of the heart on human body
b. name coverings of the heart
c. name layers of the heart wall
d. name chambers of heart and describe their functions
e. name valves of heart and describe the sounds produced by them
f. name different types of blood vessels and describe coronary circulation
g. name parts of blood
h. demonstrate how to trace pathway of blood through the heart
i. demonstrate an understanding of pulse and blood pressure
j. identify key risk factors for developing atherosclerosis and describe conditions associated with atherosclerosis within the coronary blood vessels
k. describe hypertension.
Lesson 1: Anatomy of the cardiovascular system
Activity
Ask students if they have ever seen the heart of a goat or cow. If they remember seeing one, ask them to describe its gross features.
Heart
The heart is a muscular organ and its structure makes it an efficient pump that works non-stop from the moment of development till death. The average human heart beating at 72 beats per minute will beat approximately 2.5 billion times if a person lives for 66 years. The heart, therefore, has to be strong to do this amount of activity.
Activity
Ask students what in their opinion is the average adult human heart rate per minute. Ask students to calculate the approximate number of heart beats throughout the lifetime of a person who lives for 66 years.
The heart is usually situated in the middle of the chest with the largest part of the heart placed slightly to the left. It rests on the upper surface of the diaphragm (diaphragm is a sheet of muscle which separates the chest cavity from the abdominal cavity), in front of the vertebral column and behind the sternum (breastbone). The apex of the heart points in an inferior (pointing down towards the left hip) direction. In normal adults, the heart weighs 250-350 g, and is about three quarters the size of a clenched fist.
Activity
Ask the students to make a clenched fist. Tell the students that in normal adults, the heart is about three quarters the size of their clenched fist.
Figures 1 & 2: Location of the heart
Activity
Press your fingers between the 5th and 6th ribs just below the left nipple, to feel your heart beating where the heart apex contacts the chest wall. A stethoscope can also be placed directly over the apex so that the heart beats can be counted.
Coverings of the heart and their functions
The heart is enclosed by a sac known as the pericardium. The pericardium has two walls:
· fibrous pericardium: this is a loose covering. It (a) protects the heart, (b) fixes it to surrounding structures and (c) prevents overfilling of the heart with blood
· serous pericardium: this has an inner and an outer membrane, with fluid in between to reduce friction during heart contractions.
Layers of the heart wall
The heart wall is composed of three layers.
(a) the outermost epicardium is the inner membrane of the serous pericardium (see above)
(b) the middle layer, the myocardium, is the muscular layer and forms the bulk of the heart. It is the layer that contracts during heartbeat
(c) the innermost layer, the endocardium (“inside the heart”). It lines the heart chambers.
Chambers (rooms) of the heart
The human heart is a shell. It has four chambers or "rooms" that fill with blood.
The atria are the two upper chambers that collect blood as it comes into the heart from different parts of the body
The ventricles are the two lower chambers that pump blood out of the heart to the lungs and other parts of the body.
The left side of the heart has one atrium and one ventricle. The right side of the heart has the other atrium and ventricle. A wall separates the right and left sides of the heart that is called septum. A valve connects each atrium to the ventricle below it.
Heart valves
Heart valves control the one way flow of blood from the atria to the ventricles and from the ventricles into the two large arteries connected to the heart.
The tricuspid valve is in the right side of the heart, between the right atrium and the right ventricle
The pulmonary valve is in the right side of the heart, between the right ventricle and the pulmonary artery, which carries impure blood to the lungs
The mitral valve is in the left side of the heart, between the left atrium and the left ventricle
The aortic valve is in the left side of the heart, between the left ventricle and the aorta, the artery that carries pure blood to the body.
Valves are like doors that open and close. They open to allow blood to flow through to the next chamber or to one of the arteries, and then they shut to keep blood from flowing backward.
When the valves open and close, they make a "lub-DUB" sound that a doctor can hear using a stethoscope.
The first sound-the "lub"-is made by the mitral and tricuspid valves closing at the beginning of systole. Systole is when the ventricles contract and pump blood out of the heart
The second sound-the "DUB"-is made by the aortic and pulmonary valves closing at beginning of diastole. Diastole is when the ventricles relax and fill with blood pumped into them by the atria.
Activity
Ask students to listen to their heartbeat with the stethoscope and note the two types of sounds made by the beating of the heart.
Figure 3: Heart and the great vessels from the outside
Figure 4: Heart and the great vessels from the inside
Blood vessels
Blood vessels are hollow tubes that carry the blood all around the body by the pumping action of the heart. They are located throughout the body. The three kinds of blood vessels are:
Arteries
The arteries carry blood away from the heart. All arteries in the body, with the exception of the pulmonary artery, carry high-oxygen (pure) blood.
The coronary arteries are the arteries that supply high-oxygen blood to the heart muscle itself.
Veins
Veins receive blood from the capillaries and transport low-oxygen (impure) blood back to the heart. All veins in the body carry low-oxygen blood from the body back to the heart with the exception of the pulmonary vein which carries high-oxygen blood from the lungs to the left atrium.
It is important that the impure blood keeps moving in the proper one way direction and not be allowed to flow backward. This is done by valves that are located inside the veins. The valves are like gates that only allow traffic (blood) to move in one direction towards the heart.
Capillaries
Capillaries are the smallest of the blood vessels. They are so small that the red blood cells need to partially fold in order to pass through them in single file. Unlike the arteries and veins, capillaries are very thin. They are so thin that red blood cells inside the capillary release their oxygen which passes through the wall and into the surrounding tissue. On the other hand waste products such as carbon dioxide can move back into the capillary blood to be carried away for removal from the body. In the capillaries, which connect the arteries to veins, the actual exchange of oxygen and carbon dioxide occurs.
Blood flows out of the heart through arteries and into capillaries. It then returns to the heart through veins. This is illustrated by the following diagram:
Activity
(Explain with the chart & diagram)
OR
Ask students to form 4 groups. 1st group should stand in the middle of the room. This is the “heart” and should be surrounded by the other three groups.
2nd group should form the arteries.
3rd group should form the veins.
4th group should form the capillaries.
Each group has to tell who are they and what their function is.
Figure 5: Blood flow
"heart: blood flow." Online Art. Encyclopædia Britannica Online. 19 Mar. 2008 <http://www.britannica.com/eb/art-88593>
Coronary circulation
Although blood fills the chambers of the heart, the heart muscle is so thick that it requires its own blood supply to deliver blood deep into it for its nutritional needs and to get rid of waste products. Coronary circulation is the circulation of blood in the blood vessels that supply high-oxygen blood to the heart muscle and take away low-oxygen blood from the heart muscle. The blood vessels are:
§ Right and left coronary arteries: deliver high-oxygen blood to the heart muscle
§ Cardiac veins: remove the low-oxygen blood from the heart muscle.
Blood
Blood is a body fluid. It is composed of:
1. Plasma: liquid part of the blood which is mainly water containing dissolved proteins, salts and many other substances; about 55% of whole blood is blood plasma. It is straw-yellow in color
2. Cells: solid parts suspended within the blood plasma.
The blood cells present in blood are the following:
· Red blood cells (also called RBCs). They are the most abundant cells in blood. They carry oxygen through the body in a substance called haemoglobin, which is an iron-containing protein
· White blood cells (they are of different types). They are part of the body's immune system and defend it against infection (by attacking infectious germs [pathogens]) and destroy and remove old or dead body cells; and
· Platelets. They are important in the clotting of blood thus preventing blood loss from the body.
Figure 6: Different blood cells present in blood
Activity or explain with chart
Ask students to form 4 groups. 1st group should stand in the middle of the room. This is the “plasma” and should be surrounded by the other three groups.
2nd group should form the red blood cells.
3rd group should form the white blood cells.
4th group should form the platelets.
Each group has to tell who are they and what their function is.
Lesson 2: Physiology of the cardiovascular system
Pathway of blood through the heart
Left side of the heart
The left side of the heart is called the systemic (whole body) circuit pump and pumps blood to the whole body.
The right and left pulmonary veins carry freshly oxygenated high-oxygen (pure) blood from the lungs to the left atrium. From the left atrium, blood moves to the left ventricle. From the left ventricle, blood is pumped out into the systemic circulation i.e. the whole body through the artery called aorta, which is the largest artery in the body.
The aorta divides, and branches out into many smaller arteries so that each region of the body has its own system of arteries supplying it with fresh, high-oxygen blood. The blood travels in the arteries and finally reaches the tiny capillaries which feed each cell of the body.
Flow Chart 1: Sequence of events in the left side of the heart
Right and Left pulmonary veins
ê
Left atrium
ê
Left ventricle
ê
Aorta
ê
Body
Right side of the heart
The right side of the heart is the pulmonary (lung) circuit pump and pumps blood to the lungs.
The superior vena cava is a large vein that carries low-oxygen blood from the upper body and inferior vena cava is a large vein that carries low-oxygen blood from the lower body to the right atrium. From the right atrium, blood is pumped into the right ventricle. From the right ventricle, blood is pumped into the pulmonary artery and then to the right and left lungs (pulmonary circulation). In the lungs, blood drops off carbon dioxide and picks up oxygen (gas exchange) to become pure oxygenated blood.
Flow Chart 2: Sequence of events in the right side of the heart
Superior vena cava and Inferior vena cava
ê
Right atrium
ê
Right ventricle
ê
Pulmonary artery
í
î
Right pulmonary artery
Left pulmonary artery
ê
ê
Right lung
Left lung
Activity
In small groups ask the students to discuss the sequence of events in the left and right sides of the heart. Students draw flow charts as above to show the sequence of events.
The illustration below shows a cross-section of a healthy heart and its inside structures. The blue arrow shows the direction in which impure (low-oxygen) blood flows from the body to the lungs. The red arrow shows the direction in which pure (high-oxygen) blood flows from the lungs to the rest of the body:
Figures 7 & 8: Pathway of blood through the heart
Activity
Take the students through Figure and discuss the pathway of blood through the heart.
Lesson 3: Practical
Vital health signs: pulse and blood pressure
The blood vessels provide two important means of measuring vital health signs: pulse and blood pressure.
Pulse or heart rate
We measure pulse or heart rate, by touching an artery. The arteries are the vessels with the "pulse". The rhythmic contraction of the artery keeps pace with the beat of the heart. At some places arteries are near the surface of the skin (cubital, radial, popliteal, femoral, carotid) while the heart is deeply protected, we can easily touch the artery and get an accurate measure of the heart's pulse.
Normal resting pulse rates
Adults and teens: 60 to 100 beats per minute (bpm)
Children between the ages of 6-10 years: 70 to 110 bpm
Infants: 150 bpm
Activity
Learn to take radial pulse
Step 1: Find your pulse
To find your radial artery (the most common point from which people take pulses), hold one hand straight out, elbow bent, palm relaxed and facing up. Raise your thumb slightly upward to create a small pocket under your thumb at the top of your wrist. Place the tips of your index and middle fingers of the other hand (do not use your thumb—it has also got a pulse and could cause counting confusion) on the pocket under your thumb. Your fingers should lay across the tendon running down your arm. Adjust your fingertips until you can feel a steady beat under the skin of your wrist.
Step 2: Count, multiply and determine pulse regularity
Get out your watch. First, take a count of how many pulse beats you feel for 30 seconds. Multiply the amount of beats by two to calculate your pulse rate per minute.
Then, keep your fingers on your pulse for another 30 seconds. Is your pulse steady and unwavering? Or is it irregular in any way? Irregularities to note include beats that come closer to the preceding beats than the following ones or abnormal pauses in between beats. These and any other irregularities should be reported to a doctor immediately.
Step 3: Take someone else's pulse
Use your new pulse-taking skills on your friends. The process of taking someone else's pulse is identical to taking your own, except that you will have both of your hands free to feel around for the rhythm. Do not use your thumbs as they will interfere even if you are taking someone else's pulse.
Figure 9: Taking someone else’s radial pulse
Blood pressure
Activity
Lead a group discussion by asking students if they know of somebody (e.g. parents, grandparents) with a high blood pressure.
Ask if the students know how the person (s) manage their high blood pressure.
Blood pressure is the force of blood pushing against the walls of arteries. We use the blood flowing through the arteries because it has a higher pressure than the blood in the veins.
Blood pressure is measured using two numbers. The first number, which is higher, is taken when the heart beats during the systole (contraction) phase. This is called systolic pressure. The second number, which is lower, is taken when the heart relaxes, between beats, during the diastole (relaxation) phase. This is the diastolic pressure. The two numbers are written one above or before the other.
It is normal for the blood pressure to increase when a person is exercising and to decrease when a person is sleeping.
Normal blood pressure:
120/80 mmHg
Types of blood pressure apparatus
Blood pressure is measured through the use of a medical instrument called a sphygmomanometer. There are three types of blood pressure apparatus: the mercury sphygmomanometer, the aneroid gauge and digital (electronic) devices. The mercury sphygmomanometer is the most reliable recorder available for the measurement of blood pressure.
Figures 10, 11 & 12: Different types of blood pressure apparatus
Mercury sphygmomanometer
Aneroid sphygmomanometer
Digital sphygmomanometer
Activity
Learn to take blood pressure
Step 1
Make your friend sitting comfortably and relaxed. Push the sleeves up or remove the shirt to reveal a naked arm as clothing can interfere with the pressure of the inflated cuff as well as hearing the sounds.
Step 2
The cuff of the sphygmomanometer is placed on the upper arm. It is centered over the brachial artery which is located in the bend of the elbow. Once the cuff is secured, raise the arm to heart level, place your arm underneath it to support it and ask the person to relax their arm.
Step 3
Palpate (feel for) the brachial pulse and place the chest piece of the stethoscope over this spot. Place the ear pieces of the stethoscope into your ears. Listen to the brachial pulse.
Step 4
Close the valve on the bladder of the cuff and begin to squeeze the bulb. Continue squeezing until the needle on the gauge reads 180 mmHg on the gauge. This closes the major arteries to the arm (that is why it is uncomfortable).
Step 5
Slowly release air by gently turning the air valve and allow the cuff to deflate by 5 mmHg/second while you listen to the artery. When you first hear the sound this is the systolic blood pressure. The sound you hear is the blood now flowing in the artery of the arm.
Step 6
Continue deflating the cuff until you no longer hear the sound. This is the diastolic blood pressure. At this point you can open the valve completely to allow the cuff to deflate rapidly. If you did not hear clearly, wait at least one minute before repeating the procedure.
Figure 13: Recording blood pressure
Lesson 4: Disease states
Atherosclerosis
This is the hardening and narrowing of arteries. It is a slow, progressive disease that starts in childhood. It is caused by the slow buildup of plaque inside the walls of the arteries. Plaque is made up of fat, cholesterol, calcium, and other substances found in blood. The buildup of plaque inside the walls of an artery narrows the inner diameter of that artery and, in time, may reduce blood flow.
Figure 14: Cut sections of a normal artery (left) and artery narrowed by atherosclerotic plaque (right)
The coronary arteries are commonly affected by atherosclerosis and can become blocked. Blocked or narrowed blood vessels cause ischaemia (inadequate supply of blood and hence of oxygen) of the heart muscle. Blockage of the coronary arterial circulation can be serious and sometimes can even cause death. Coronary artery disease causes:
• Angina pectoris
• Myocardial infarction
• Sudden death
Activity
Look at the above figure and discuss the difference between the arteries and its impact on the person’s health.
Angina pectoris
Commonly known as angina, it is chest pain due to temporary ischaemia of the heart muscle. Muscle cells are weakened by the temporary lack of oxygen but do not die. Major risk factors for angina include cigarette smoking, diabetes, high cholesterol, high blood pressure, lack of exercise and family history of premature heart disease.
Angina typically happens by physical exertion or emotional stress. It is worsened by having a full stomach and by cold temperatures. It usually lasts for about 1 to 5 minutes, and is relieved by rest or specific anti-angina medication. Chest pain lasting only a few seconds is normally not angina.
Symptoms of angina
· Chest pain OR chest discomfort: this is described as a pressure, heaviness, tightness, squeezing, burning, or choking sensation
· Pain in the epigastrium (upper central abdomen), back, neck, jaw, or shoulders
· Pain from the chest may spread into arms (often inner left arm), shoulders, and neck into the jaw
· Breathlessness, sweating and nausea (in some cases)
Myocardial infarction (heart attack)
Acute myocardial infarction (tissue death due to oxygen starvation), more commonly known as a heart attack, is a condition that occurs when the blood supply to a part of the heart is interrupted. The resulting ischaemia or oxygen shortage causes damage and death of heart muscle. It is a medical emergency, and the leading cause of death for both men and women all over the world.[1]
1. The World Health Report 2004 - Changing History (PDF), World Health Organization, 120-4. ISBN 92-4-156265-X.
Risk factors are a previous history of coronary heart disease and/or angina, a previous heart attack or stroke, older age—especially men over 40 and women over 50, smoking, excessive alcohol intake, high triglycerdies, high LDL ("Low-density lipoprotein") and low HDL ("High density lipoprotein"), diabetes, high blood pressure, obesity, and chronically high levels of stress.
Symptoms of acute myocardial infarction
Men:
· Chest pain (typically spreading to the left arm)
· Shortness of breath
· Nausea, vomiting
· Palpitations
· Sweating
· Anxiety
Women: may have different symptoms from men
· Shortness of breath
· Weakness
· Lack of muscle strength
Note: Nearly one third of all myocardial infarctions are silent, without chest pain or other symptoms
Figure 15: Heart, part of which is dead after a heart attack
Activity
Brainstorm what is happening in the above figure.
Hypertension
Hypertension (high blood pressure) is a condition in which the blood pressure is chronically elevated. Hypertension means when a person's systolic blood pressure is consistently 140 mmHg or higher, and/or their diastolic blood pressure is consistently 90 mmHg or higher.
Hypertension is of two types:
1. Essential (primary) hypertension: in this type there is no specific medical cause not yet known
2. Secondary hypertension: in this type, the high blood pressure is a result of another condition, such as kidney disease or certain tumors producing chemicals that may increase the blood pressure.
High blood pressure usually has no symptoms, but it can cause serious problems such as strokes, heart attacks, heart failure, and kidney failure. Even moderate increase of blood pressure leads to a shortened life and so every effort should be done to maintain normal blood pressure.
High blood pressure can be controlled through healthy lifestyle habits such as daily exercise, low sodium diet, low fat diet, loss of weight and taking medicines, if needed.
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: Human body
Sub-unit 2.1 Date: ________________________
Describe the location and position of the heart in the body.
________________________________________________________________________________________________________________________________________________________________________________________________________________________
The heart wall is composed of the following three layers:
a. ______________________________________________________________________
b. ______________________________________________________________________
c_______________________________________________________________________
The four chambers of heart are
a. ____________________________________________________________________
b. ____________________________________________________________________
c. ____________________________________________________________________
d. ____________________________________________________________________
Trace one drop of blood from the time it enters the right atrium until it enters the left atrium.
________________________________________________________________________________________________________________________________________________
What is the function (job) of the coronary artery?
________________________________________________________________________
Normal blood pressure is___________________mmHg
The pulse is most commonly felt in the ______________ artery in the arm.
Blood consists of
a. _________________________________________________________
b.__________________________________________________________
The pericardium is composed of (circle one)
a. Two walls
b. Three walls
c. Four layers
Freshly oxygenated blood is first received by the (circle one)
a. Right atrium
b. Left atrium
c. Right ventricle
d. Left ventricle
The right atrium is connected with the right ventricle by (circle one)
a. Aortic valve
b. Pulmonary valve
c. Tricuspid valve
d. Mitral valve
Blood leaves the left ventricle through (circle one)
a. Inferior vena cava
b. Pulmonary artery
c. Aorta
d. Pulmonary vein
Pulmonary arteries carry (circle one)
a. oxygen-poor blood.
b. oxygen-rich blood.
c. oxygen-neutral blood.
Deoxygenated blood is oxygenated in (circle one)
a. Lungs
b. Right atrium
c. Left atrium
d. Left ventricle
The arteries carry blood (circle one)
a. away from the heart
b. towards the heart
Arteries are blood vessels that typically carry blood away from the (circle one)
a. heart to the body and lungs
b. body and lungs to the heart
c. right lung to the left lung and heart
Veins are blood vessels that carry blood (circle one)
a. away from the heart
b. towards the heart
The science term for the heart attack is (circle one)
a. Angina
b. Angina pectoris
c. Myocardial infarction
The most abundant cells in blood are (circle one)
a. Leukocytes
b. Lymphocytes
c. Red blood cells
d. Platelets
Pain of myocardial infarction can get relieved by rest
True False
Sub-unit 2.2
The Gastrointestinal System
Learning objectives:
After completing sub-unit 2.2 dispenser students will be able to:
a. describe gross anatomy of the digestive system
b. describe basic functions of various parts of the digestive system
c. demonstrate an understanding of lower GI tract for administering enemas and suppositories and passing flatus tubes
d. mark location of stomach, liver and appendix on human body
e. identify and recognize signs of dehydration
f. demonstrate how to guide clients about oral rehydration therapy and hygiene
g. demonstrate an understanding of relationship of digestive system with food and water in the context of disease generation and propagation.
Introduction
The digestive system takes in food, breaks it down into nutrient molecules, absorbs these molecules into the blood stream, and then rids the body of the indigestible remains.
Lesson 1: Anatomy of the digestive system
Activity
Ask students if they have ever seen the digestive tract of a goat or cow. If they remember seeing one, ask them to describe its gross features.
The organs of the digestive system fall into two groups:
Gastrointestinal tract:
It is a continuous, muscular tube that winds through the body. It can be divided into:
· Upper gastrointestinal tract: this consists of the mouth, pharynx, esophagus, and stomach
· Lower gastrointestinal tract: this consists of the small intestine and large intestine.
Upper gastrointestinal tract
This consists of the mouth, pharynx, esophagus, and stomach.
The mouth is a cavity with its boundaries being the lips at the front, cheeks on the sides, hard and soft palate above, and tongue below. At the back it is continuous with the oropharynx, which is part of pharynx.
The pharynx (throat) is situated immediately behind the mouth and nasal cavity. It is about 13 cm long. The pharynx is part of the digestive system as well as the respiratory system because it carries both food and air. Epiglottis protects air passage during swallowing.
The esophagus (food pipe) is a muscular tube through which food passes from the pharynx to the stomach.
The stomach lies between the esophagus and the duodenum (the first part of the small intestine). It is on the left side of the abdominal cavity. The top of the stomach lies against the diaphragm. Lying beneath the stomach is the pancreas. In humans, the stomach has a volume of about 50 ml when empty. After a meal, it generally expands to hold about 1 liter of food, but can hold as much as four liters.
Lower gastrointestinal tract
This consists of the small intestine and large intestine.
The small intestine lies between the stomach and the large intestine and is approximately 7 m long. Although the small intestine is much longer than the large intestine, it is referred to as such due to its comparatively smaller diameter. The vast majority of digestion takes place in the small intestine. It is made up of three parts:
duodenum: the C-shaped first part; it curves around the head of the pancreas
jejunum: the coiled midsection; and
ileum: the final section that leads into the large intestine.
The large intestine is the last part of the digestive system. It is about 1.5 meters long and is made up of the following parts:
cecum: the first part of large intestine is a pouch at the beginning of the large intestine that joins the small intestine to the colon. The appendix, a small, hollow, finger-like pouch, hangs at the end of the cecum.
colon: is divided into ascending colon (which goes up the right side of the abdomen), transverse colon (which runs across the upper abdomen), descending colon (which runs down the left side of the abdomen), and sigmoid colon (after the descending colon and before the rectum).
rectum: it is connected above with the sigmoid colon and with the anal canal below. This is where faeces are stored until they leave the digestive system through the anus.
anal canal: it is situated between the rectum and anus (the external opening of the rectum).
Figure 1 - Parts of the large intestine
Accessory digestive organs: These are the teeth, tongue, salivary glands, gallbladder, liver and pancreas which are not part of the gastrointestinal tract, but are essential to digestion.
Salivary glands are located under the tongue and near the lower jaw
Liver is located under the rib cage in the right upper part of the abdomen
Gallbladder lies hidden just below the liver; and
Pancreas lies beneath the stomach.
Figure 2- Gastrointestinal tract and accessory digestive organs
Figure 3 - Gastrointestinal tract and accessory digestive organs and details of intestinal sections
Figure 4: Gastrointestinal tract
Activity
Have a look at Figure 2, 3, 4 and 5. With the help of a chalk, mark the location of stomach, liver and appendix on your friend’s body.
Figure 5: Location of stomach in the body
Figure 6: Location of liver in the body
Figure 7 - Location of appendix in the body
Lesson 2: Physiology of the digestive system
Digestion
Digestion in the mouth
Digestion begins in the mouth, well before food reaches the stomach. When we see, smell, taste, or even imagine good food, a brain reflex is triggered; in response to this sensory stimulation, the brain sends impulses through the nerves that control the salivary glands in the mouth, telling them to prepare for a meal and our salivary glands begin producing saliva.
As the teeth chop the food, saliva moistens it for easy swallowing. A digestive enzyme, amylase (enzymes are proteins that speed up chemical reactions) found in saliva, starts to break down some of the carbohydrates (starches and sugars) in the food even before it leaves the mouth.
Swallowing, which is accomplished by muscle movements in the tongue and mouth, moves the food into the pharynx. Epiglottis reflexively closes over the trachea (windpipe) when we swallow to prevent choking.
Digestion in the stomach
From the throat, food travels down the esophagus. Waves of muscle contractions called peristalsis force food down through the esophagus to the stomach. A person normally is not aware of the movements of the esophagus, stomach, and intestine that take place as food passes through the digestive tract.
At the end of the esophagus, a muscular valve called a sphincter allows food to enter the stomach and then squeezes shut to keep food or fluid from flowing back up into the esophagus. The stomach muscles churn and mix the food with acids and enzymes, breaking it into much smaller, digestible pieces. An acidic environment is needed for the digestion that takes place in the stomach. Glands situated in the stomach lining produce about 2.8 liters of digestive juices each day (pepsin and Hydrochloric acid). By the time food is ready to leave the stomach, it has been processed into a thick liquid called chyme. A muscular valve at the outlet of the stomach called the pylorus keeps chyme in the stomach until it reaches the right consistency to pass into the small intestine. Chyme is then moved down into the small intestine
Digestion in the small intestine
Most substances in the food we eat need further digestion and must travel into the intestine before being absorbed. In the small intestine, digestion of food continues so the body can absorb the nutrients into the bloodstream. The inner wall of the small intestine is covered with millions of microscopic, finger-like projections called villi. The villi are the sites through which nutrients can be absorbed into the body. (bile & juices)
Digestion in the large intestine
From the small intestine, undigested food (and some water) travels to the large intestine through a valve that prevents food from returning to the small intestine. By the time food reaches the large intestine, the work of absorbing nutrients is nearly finished. Bacteria in the colon help to digest the remaining food products. The large intestine's main function is to remove water by absorption from the undigested matter and form solid waste that can be excreted.
Role of liver and pancreas in digestion
Both liver and pancreas help to break down food in different ways: liver secretes bile into the small intestine; bile which helps the body absorb fat is first stored in the gallbladder where it is also concentrated and then it is released into the small intestine. Apart from storing and concentrating bile, the gallbladder has no other specific function. The liver also plays a major role in the handling and processing of nutrients, which are carried to the liver in the blood from the small intestine. The pancreas secretes several enzymes for digesting protein, fat and carbohydrates into the small intestine. The pancreas also secretes bicarbonate for neutralizing stomach acid.
Activity
Ask students to form 4 groups:
1st group is “Digestion in the mouth”.
2nd group is “Digestion in the stomach”.
3rd group is “Digestion in the small intestine”.
4th group should assume the “Role of liver and pancreas in digestion”
Each group has to tell who are they? (all organs in that group) and what their function(s) is?
Lesson 3: Disease states
Waterborne diseases
Water-borne diseases are any illness caused by drinking contaminated water, which contains disease-causing germs.
In developing countries like Pakistan, four-fifths of all the illnesses are caused by water-borne diseases, with diarrhoea being the leading cause of childhood death. According to the World Health Organization, diarrheal disease is responsible for the deaths of 1.8 million people every year. It was estimated that nearly 90% of that burden is attributable to unsafe water supply, sanitation and hygiene, and is mostly concentrated in children in developing countries.[1]
1. WHO. Burden of disease and cost-effectiveness estimates. 2004
Activity
Brainstorm the reasons of water contamination in Pakistan.
Transmission
Water-borne diseases spread by contamination of drinking water systems with the urine and faeces of infected animal or people. This is likely to occur where public and private drinking water systems get their water from surface waters (rain, creeks, rivers, lakes etc.), which can be contaminated by infected animals or people. Runoff from landfills, septic fields, sewer pipes, residential or industrial developments can also sometimes contaminate surface water. The germs in the faeces can cause the disease by even slight contact and transfer.
The only way to break the continued transmission is to improve the people’s hygienic behavior and to provide them with certain basic needs: drinking water, washing and bathing facilities and sanitation. Malaria transmission is facilitated when large numbers of people sleep outdoors during hot weather, or sleep in houses that have no protection against invading mosquitoes. Malaria mosquitoes, tropical black flies, and bilharzias snails can all be controlled with efficient drainage because they all depend on water to complete their life cycles.
Causes of Waterborne Diseases
These can be caused by protozoa, viruses, bacteria, and intestinal parasites.
Protozoa
Amoebiasis - Entamoeba histolytica
Viruses
Hepatitis A - Hepatitis A virus
Polio - polioviruses
Bacteria
Botulism - Clostridium botulinum
Cholera - Vibrio cholera
Gastroenteritis (diarrheal disease) - E. coli
Dysentery - Shigella/Salmonella
Typhoid - Salmonella typhi.
Intestinal parasites
Enterobiasis - Entrobius vermicularis
Prevention
Clean water is a pre-requisite for reducing the spread of water-borne diseases. It is well recognized that the prevalence of water-borne diseases can be greatly reduced by provision of clean drinking water and safe disposal of feces.
Water is disinfected to kill any germs that may be present in the water supply and to prevent them from growing again in the distribution systems. Without disinfection, the risk from waterborne disease is increased. The two most common methods to kill germs in the water supply are: oxidation with chemicals such as chlorine, chlorine dioxide or ozone, and irradiation with Ultraviolet (UV) radiation.
Food-borne diseases
Activity
Brainstorm the reasons of food contamination in Pakistan.
Food-borne disease is any illness caused by eating contaminated foods or beverages. More than 250 different food-borne diseases have been seen. Many different disease-causing germs - bacteria, viruses, and parasites - can contaminate food. In addition, poisonous chemicals, or other harmful substances can also cause food-borne diseases if they are present in food. For example people can become ill if a pesticide is inadvertently added to a food, or if naturally poisonous substances e.g. poisonous mushrooms are used to prepare a meal.
Food borne disease is commonly called food poisoning, even though it is not always caused by poisons. Food contamination usually arises from improper handling, preparation, or food storage. Good hygiene practices before, during, and after food preparation can reduce the chances of getting an illness. Food borne diseases remain responsible for high levels of morbidity and mortality in the general population, but particularly for at-risk groups, such as infants and young, children, and the elderly.
These different food borne diseases have many different symptoms. However, the germs or poisons enter the body through the gastrointestinal tract, and often cause the first symptoms there, so nausea, vomiting, abdominal pain and diarrhea are common symptoms in many food borne diseases. After the contaminated food is swallowed, there is a delay before the symptoms of illness begin. This delay may range from hours to days, depending on the germ, and on how many of them were swallowed. During this time, the germs pass through the stomach into the intestine, attach to the cells lining the intestinal walls, and begin to multiply there. Some types of germs stay in the intestine, some produce a toxin that is absorbed into the bloodstream, and some can directly invade the deeper body tissues.
The most commonly recognized food borne infections are those caused by the bacteria Campylobacter, Salmonella, and E. coli, and by a group of viruses called the Norwalk viruses.
Campylobacter is the most commonly identified bacterial cause of diarrheal illness in the world. These bacteria live in the intestines of healthy birds, and most raw poultry meat has Campylobacter on it. Eating undercooked chicken is the most frequent source of this infection.
Salmonella can spread to humans via a variety of different foods of animal origin. In persons with poor underlying health, it can invade the bloodstream and cause life-threatening infections.
E. coli has a reservoir in cattle and other similar animals. Human illness typically follows consumption of food or water that has been contaminated with microscopic amounts of cow feces.
Norwalk-like virus is an extremely common cause of food borne illness. Unlike many food borne germs that have animal reservoirs, it is believed that these viruses spread primarily from one infected person to another.
In addition to disease caused by direct bacterial infection, some food borne illnesses are caused by poisons which are excreted by the bacterium as it grows. These poisons can produce illness even when the germs that produced them have been killed. E.g. the bacterium Staphylococcus aureus produces a poison that causes intense vomiting.
Dehydration
Dehydration means the body does not have as much water and fluids as it should. Dehydration can be caused by losing too much fluid, not drinking enough water or fluids, or both. Vomiting and diarrhea (watery stools) are common causes.
In diarrhea, muscle contractions move the contents of the intestines along too quickly and there is not enough time for water to be absorbed before the feces are pushed out of the body. Gastrointestinal infections caused by viruses, bacteria (such as Salmonella, Shigella, Campylobacter, or E. coli), or by intestinal parasites (such as amoebiasis) are a common cause of diarrhea, abdominal pain, and sometimes vomiting.
Infants and children are more susceptible to dehydration than adults because of their smaller body weights and higher turnover of water and electrolytes. The elderly and those with illnesses are also at higher risk.
Dehydration is classified as mild, moderate, or severe based on how much of the body's fluid is lost or not replaced. When severe, dehydration is a life-threatening emergency. When dehydration is recognized and treated promptly, the outcome is generally good. Untreated severe dehydration may result in fits, permanent brain damage, or death.
Causes
Body may lose too much fluid from:
Vomiting or diarrhea
Excessive urine output, such as with uncontrolled diabetes or diuretic use
Excessive sweating (for example, from exercise)
Fever
A person might not drink enough fluids because of:
Nausea
Loss of appetite due to illness
Sore throat or mouth sores
Dehydration in sick children is often a combination of both - refusing to eat or drink anything while also losing fluid from vomiting, diarrhea, or fever.
Symptoms of dehydration
· Dry or sticky mouth
· Low or no urine output; concentrated urine appears dark yellow
· Not producing tears
· Sunken eyes
· Depressed soft-spot on the top of an infant's head
· Lethargic or comatose (with severe dehydration)
Signs of dehydration
· Low blood pressure
· Blood pressure that drops when the patient stands up from a lying position
· Rapid heart rate
· Poor skin elasticity - dry skin that sags back into position slowly when pinched up into a fold; normally, skin springs right back into position
· Delayed capillary nail refill (pressure is applied to the nail bed until it turns white, indicating that the blood has been forced from the tissue. Once white, pressure is removed. It will take longer than normal for the nail bed to turn pink)
· Shock
Treatment Mild dehydration
During diarrheal disease, for example due to cholera or some virus, the volume of intestinal fluid output is substantially increased, and is more than the reabsorptive capacity of the gastrointestinal tract. In addition, electrolytes such as sodium (Na+) and potassium (K+) are also lost in huge amounts in diarrhea.
Giving a saline solution (water plus Na+) by mouth has no beneficial effect because the normal mechanism by which Na+ is absorbed by the healthy intestinal wall is impaired in the diarrheal state and if the Na+ is not absorbed neither can the water be absorbed. In fact, excess Na+ in the lumen of the intestine causes increased secretion of water and the diarrhea worsens.
If glucose is added to a saline solution a new mechanism comes into play. The glucose molecules are absorbed through the intestinal wall - unaffected by the diarrheal disease state - and in conjunction sodium is carried through by a co-transport coupling mechanism. This occurs in a 1:1 ratio, one molecule of glucose co-transporting one sodium ion (Na+).
The most crucial aspect underlying home management of diarrhea is the need to replace fluid losses and to maintain adequate nutrient intake. Regardless of the fluid used, an age-appropriate diet should also be given. Infants should be offered more frequent breast or bottle feedings, and older children should be given more fluids.
Oral rehydration therapy (ORT) is a simple, cheap, and effective treatment for diarrhea-related dehydration. ORT includes rehydration and maintenance fluids with oral rehydration solutions (ORS), combined with continued age-appropriate nutrition.
Treatment with ORS is simple and enables management of uncomplicated cases of diarrhea at home, regardless of causative agent. As long as caregivers are instructed properly regarding signs of dehydration or are able to determine when children appear markedly ill or appear not to be responding to treatment, therapy should begin at home. Early intervention can reduce such complications as dehydration, malnutrition, and death.
Adults and children with dehydration who are not vomiting can be allowed to drink these solutions in addition to their normal diet. People who are vomiting should be fed small frequent amounts of ORS solution until dehydration is resolved. Once they are rehydrated, they may resume eating normal foods.
All families should be encouraged to have a supply of ORS in the home at all times and to start therapy with a commercially available ORS as soon as diarrhea begins. Although producing a homemade solution with appropriate concentrations of glucose and sodium is possible, serious errors can occur; thus, standard commercial oral rehydration preparations should be recommended.
Vomiting itself does not mean that ORT cannot be given. As long as more fluid enters than leaves the body, rehydration will be accomplished. It is only when the volume of fluid and electrolyte lost in vomit and stool exceeds what is taken in, that dehydration will continue.
WHO (2004) recipe for home-made ORS
To one liter of clean drinking or boiled and cooled water add:
§ Salt ½ small spoon (3.5 grams)
§ Sugar 4 big spoons (40 grams)
The standard, manufactured WHO/UNICEF glucose-based ORS solution
§ Sodium Chloride 3.5 grams
§ Sodium Bicarbonate 2.5 grams
§ Potassium Chloride 1.5 grams
§ Glucose 20 grams t
To be added to one litre of clean drinking or boiled and cooled water
Ten things you should tell the caregiver who is rehydrating a child
i. Wash your hands with soap and water before preparing solution.
ii. Prepare a solution, in a clean pot, by mixing
· ½ small spoon salt and 4 big spoons sugar or 1 packet of ORS, with one liter of clean drinking or boiled water (after being cooled)
· Stir the mixture till all the contents dissolve.
iii. Wash your hands and the child’s hands with soap and water before feeding solution.
iv. Give the sick child as much of the solution as needed, in small amounts frequently.
v. Give child alternately other fluids - such as breast milk and juices.
vi. Continue to give solids if child is four months or older.
vii. If the child still needs ORS after 24 hours, make a fresh solution.
viii. ORS does not stop diarrhea. It prevents the body from drying up. The diarrhea will stop by itself.
ix. If child vomits, wait ten minutes and give ORS again. Usually vomiting will stop.
x. If diarrhea increases and /or vomiting persist, take child over to a health clinic.
Moderate to severe dehydration
Intravenous fluids and hospitalization may be necessary for moderate to severe dehydration.
Malnutrition
Malnutrition is a general term for a medical condition caused by an improper or insufficient diet. An individual will experience malnutrition if the appropriate amount of, or quality of nutrients comprising a healthy diet are not consumed for an extended period of time. An extended period of malnutrition can result in starvation, disease, and infection. Most commonly, malnourished people either do not have enough calories in their diet, or are eating a diet that lacks protein, vitamins, or other necessary substances.
Types of Malnutrition
There are two types of malnutrition:
i. Under-nutrition: this results from inadequate consumption, poor absorption, or excessive loss of nutrients. Malnutrition is the lack of sufficient nutrients to maintain healthy bodily functions and is typically associated with extreme poverty in the developing countries.
ii. Over-nutrition: this results from overeating or excessive intake of specific nutrients. Malnutrition as the result of inappropriate dieting, overeating or the absence of a "balanced diet" is often observed in the developed countries (eg. as indicated by increasing levels of obesity).
Causes of malnutrition
Famine
Poverty
Overpopulation
Diseases of the gastrointestinal tract
Malabsorption (abnormality in digestion or absorption of food nutrients across the gastrointestinal tract)
Depression
Untreated diabetes mellitus
Fasting
Coma
Alcoholism and other certain drug addictions
Over-consumption of fat and sugar
Eating of processed food (fast food)
In 2001-2003, the number of undernourished people in Pakistan were 35.2 million.
(The Food and Agriculture Organization of the United Nations)
Lesson 4: Practical
Activity
With the materials provided, prepare an oral rehydration solution.
Role play
· The role play involves two students:
· One student is to play the role of a dispenser who is being visited by the parent of a small child who is dehydrated due to diarrhoea.
· The other student is to play the role of the parent.
· The two students should discuss the ten things related to oral rehydration therapy.
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: Human body
Sub-unit: 2.2 Date: _________________________
The esophagus connects ____________with ______________.
Lying beneath the stomach is (circle the 1 correct answer)
a. Pancreas
b. Duodenum
c. Liver
d. Gall bladder
Lower gastrointestinal tract can be divided into:
a. _________________________________
b. _________________________________
Small intestine is made of the following three parts: (circle the 3 correct answers)
a. Duodenum
b. Jejunum
c. Cecum
d. Ileum
Digestion starts in the mouth
True False
Bile is secreted by (circle the correct answer)
a. Gall bladder
b. Pancreas
c. Liver
d. Appendix
The function of the gall bladder is to
a. _________________________________
b. _________________________________
The signs of dehydration are:
a. _________________________________
b. _________________________________
c. _________________________________
d. _________________________________
e. _________________________________
Home-made oral rehydration solution can be made by adding the following two ingredients to one litre of clean drinking water
a. _________________________________
b. _________________________________
Label the following diagram of the digestive system
Notes
Sub-unit 2.3
Pulmonary System
Learning objectives:
After completing sub-unit 2.3 dispenser students will be able to:
describe gross anatomy of the pulmonary system
describe basic functions of various parts of the pulmonary system
mark location of lungs on human body
d. identify signs and symptoms of pneumonia and pulmonary tuberculosis
Lesson 1: Anatomy of the System
The respiratory system is divided into:
i. The upper respiratory tract
· nose
· pharynx
· larynx
ii. The lower respiratory tract
· trachea
· bronchi
· bronchioles
· lungs
· alveoli within the lungs.
i. Upper respiratory tract
Nose: it is the only externally visible part of the respiratory system and is divided into the outer nose and the inner nasal cavity. Nose performs the following functions:
air enters the respiratory system through the nose
it filters and cleans the inhaled air so that air entering the lungs has fewer irritants (dust, bacteria etc) than when it entered the nose
it moistens and warms the inhaled air
it provides resonance in speech
smell receptors are located in the nose.
Pharynx (throat): it is situated immediately behind the nasal cavity and mouth. It is about 13 cm long. The pharynx is part of the digestive system as well as the respiratory system because both food and air pass through it. At the bottom of the pharynx, this common pathway splits, with one pathway for food (called the esophagus, which leads to the stomach) and the other (called the trachea, which leads to the lungs) for air. The epiglottis, a small flap of tissue, covers the air-only pipe (trachea) when we swallow, keeping food and liquid from going into our lungs and prevents choking. At the back of the mouth, on each side of the throat, lie the tonsils.
Larynx (voice box): it is the uppermost part of the air-only pipe; it opens above into the pharynx and below it is continuous with the trachea. This short tube contains a pair of vocal cords, which vibrate to make sounds.
ii. Lower respiratory tract
Trachea (windpipe): it is a tube that lies partly in the neck and partly in the chest cavity. The trachea begins at the lower part of the larynx and continues to the lungs, where it ends by dividing into the right and left main bronchi. It is 10-12 cm long and 2.5 cm in diameter. The trachea is lined with cilia (hair-like structures), which sweep fluids and foreign particles out of the airway so that they stay out of the lungs.
Bronchi, Bronchioles, and Alveoli: at its bottom end the trachea divides into the right and left air tubes called primary bronchi, which connect to the lungs. Once inside the lungs, each primary bronchus subdivides into smaller bronchi (secondary and tertiary) which in turn branch into even smaller bronchi called bronchioles. Bronchioles end in tiny air sacs called alveoli, where the exchange of oxygen and carbon dioxide actually takes place. Each lung has about 300 to 400 million gas-filled alveoli. This network of alveoli, bronchioles, and bronchi is known as the bronchial tree.
Lungs: they are the essential respiration organ and serve as the gas-exchanging organ for the process of respiration. They provide us with a continuous flow of oxygen and clear the blood of the gaseous waste product, carbon dioxide.
The two lungs are located in the chest on either side of the heart. The lungs are divided into lobes and work closely with the heart. The lungs are surrounded by two membranes called the pleurae. Between the two membranes is a thin space known as the pleural space, which normally contains a small amount of fluid. The pleura acts to protect the lungs.
Besides the bronchial tree, the lungs also contain elastic tissues that allow them to inflate and deflate without losing shape.
Figure 1: Respiratory system
Figure 2: Respiratory system showing details of bronchioles and alveoli
Figure 3: Bronchi, bronchial tree and lungs
Figure 4: Bronchial tree
Figure 5: Alveoli
Activity
Have a look at Figure 6. With the help of a chalk, mark the position of the lungs on your friend’s body.
Figure 6: Location of right and left lungs in the human body
Lesson 2: Physiology of the respiratory system
Respiration
The major function of the respiratory system is respiration (breathing) by which the body is supplied with oxygen and disposed of carbon dioxide. Each day we breathe in about 20,000 times and by the time we are 70 years old, we will have taken at least 600 million breaths.
Breathing is an active process - requiring the contraction of skeletal muscles (see Unit 2, Sub-unit 2.4, Musculoskeletal System and Skin).
Breathing consists of two phases:
i. Inhalation phase. Inhalation allows air (oxygen) to flow into the lungs; the chest muscles and diaphragm contract allowing air to enter the lungs as follows:
Contraction of chest muscles è elevation of ribs and sternum è increased front- to-back dimension of chest cavity è lowers air pressure in lungs è air moves into lungs
Contraction of diaphragm è diaphragm moves downward è increases vertical dimension of chest cavity è lowers air pressure in lungs è air moves into lungs
ii. Exhalation. Exhalation involves gases (carbon dioxide) leaving the lungs; the chest muscles relax forcing gases to flow out of the lungs as follows:
Relaxation of chest muscles and diaphragm è return of diaphragm, ribs, and sternum to resting position è restores chest cavity to pre-inspiratory volume è increases pressure in lungs è air moves out of lungs (air is exhaled).
Pathway of air through the lungs
Nasal cavities (or mouth cavity) è pharynx è trachea è primary bronchi (right and left) è secondary bronchi è tertiary bronchi è bronchioles è alveoli (site of gas exchange).
With every breath, we inhale (breathe in) oxygen-rich air through our nose and mouth and our lungs fill up. Oxygen passes out of the lungs into the tiny blood vessels called capillaries found deep within the lungs. Once in the bloodstream, oxygen binds to red blood cells, and high-oxygen blood (oxygenated blood) from the lungs goes to the left side of the heart via the right pulmonary vein and left pulmonary vein. The left ventricle pumps the high-oxygen blood out to all parts of the body via the aorta.
Body cells use the oxygen from the blood and release the waste gas - carbon dioxide, which is carried back in low-oxygen blood through superior vena cava and inferior vena cava to the right side of the heart. The right ventricle pumps low-oxygen blood through right and left pulmonary arteries to the lungs, where carbon dioxide is released and exhaled (breathed out). (See Unit 2, sub-unit 2.1, Cardiovascular System)
The principal function of the lungs is to transport oxygen from the atmosphere into the bloodstream, and to release carbon dioxide from the bloodstream into the atmosphere. The exchange of gases (O2 and CO2) between the alveoli and the blood occurs by simple diffusion: O2 diffusing from the alveoli into the blood and CO2 from the blood into the alveoli. Diffusion requires a difference in pressure. So, the concentration (or pressure) of O2 in the alveoli must be kept at a higher level than in the blood and the concentration (or pressure) of CO2 in the alveoli must be kept at a lower lever than in the blood. We do this by breathing - continuously bringing fresh air (with lots of O2 and little CO2) into the lungs and the alveoli.
The lungs' ability to stretch and then return to their original shape after expiration is crucial to the process of breathing because without doing so, there would be no air movement. When the lungs cannot exhale enough carbon dioxide, a toxic buildup occurs, poisoning all the cells of the body. Any factor that causes the airways to constrict or narrow, or which causes the lungs to become less resilient, will increase the work of breathing.
Figure 7: The process of Inhalation and Exhalation
Activity:
Look at Figure 8 and differentiate between the two men noting the following points:
Position of rib cage
Size of lungs
Position of diaphragm (red).
Figure 8: The process of inspiration (Inhalation) and expiration (Exhalation)
Lesson 3: Disease states
Pneumonia
It is defined as an inflammation of the lung. Inflammation produces areas of the lung that are stiff and full of fluid, called consolidation.
Pneumonia is a common illness which occurs in all age groups and is a leading cause of death among the elderly. If a patient with pneumonia was previously well, with treatment, they are likely to make a full recovery. However, some bacteria, viruses, and other germs are more serious than others making some people become very ill and requiring hospital admission. Occasionally, some people who were previously well die from pneumonia.
If the patient was already in poor health, they are more likely to become seriously ill with pneumonia. Pneumonia is a common cause of death in people who are already in poor health. For example, people in the late or terminal stages of a cancer.
Causes
Infection with bacteria or viruses. Other germs such as fungi, or parasites may also cause pneumonia
Inhalation of poisons or chemicals
Physical injury to the lungs.
How does pneumonia occur?
A person may breathe-in some bacteria, viruses, or other germs. If the person is normally healthy, a small number of germs usually does not matter as they are trapped in the sputum and are killed by the immune system. If a person is already in poor health e.g. if they are frail or elderly, have a chest disease, or have a low immunity to infection because of AIDS or another serious illness, the germs multiply and cause lung infections. However, even healthy people sometimes develop pneumonia
Common signs and symptoms
§ Cough producing greenish or yellow sputum
§ Blood in sputum
§ Chest pain - a sharp or stabbing pain, either felt or worse during deep breaths or coughs
§ Headaches
§ Sweaty and clammy skin
§ High fever that may be accompanied by shaking chills or low body temperature
§ Difficulty in breathing.
§ An increased respiratory rate
§ Low blood pressure
§ A fast heart rate
Other symptoms
§ Loss of appetite
§ Fatigue
§ Blueness of the skin
§ Nausea, vomiting
§ Joint pains or muscle aches
Infants with pneumonia may have many of the symptoms above, but in many cases they are simply sleepy or have a decreased appetite.
Diagnosis
Pneumonia is usually diagnosed based on symptoms and findings from physical examination. Information from a chest X-ray, blood tests, and sputum cultures may also be helpful. Diagnosing pneumonia can be difficult in some people, especially those who have other illnesses.
Physical examination: Areas of consolidation can be identified by auscultation, palpation and percussion:
Auscultation (listening to the lungs with a stethoscope) can reveal several things - a lack of normal breath sounds, the presence of crackling sounds, or increased loudness of whispered speech.
Palpation is done to feel the way the chest expands and for increased vibration of the chest when speaking, and
Percussion is done by tapping the chest wall to further localize consolidation.
Chest x-ray: Useful in unclear situations. Chest x-rays can reveal white areas which represent consolidation and where there is no air. Pneumonia is not always seen on x-rays, either because the disease is only in its initial stages, or because it involves a part of the lung not easily seen by x-ray.
Figure 9: A: Normal chest x-ray. B: Abnormal chest x-ray with areas of consolidation in the right lung (white area, left side of image).
Sputum culture: If antibiotics fail to improve the patient's health, or if the health care provider has concerns about the diagnosis, a culture of the person's sputum may be requested. Sputum cultures generally take at least two to three days, so they are mainly used to confirm that the bacteria are sensitive to the antibiotic that has already been started.
Blood tests: A complete blood count may show a high white blood cell count, indicating the presence of an infection. Blood culture may be done to look for infection in the blood Any bacteria identified are then tested to see which antibiotics will be most effective.
Treatment
If the pneumonia is not too severe, treatment at home may be fine if the patient is normally healthy.
Antibiotics are prescribed when pneumonia is suspected. Bacterial infection is the common cause of pneumonia and antibiotics kill bacteria. Antibiotic treatment usually works well, and patient can expect to fully recover. Symptoms settle over a few days if the treatment is working though the patient may feel tired for a week or so after the infection has cleared.
Have lots to drink to avoid dehydration.
Take regular paracetamol or ibuprofen to ease fever and pain.
Stronger painkillers may be required if chest pain develops due to an inflamed pleura (pleurisy).
Patient should come back for a follow-up if symptoms do not improve over the next two days.
If the patient has severe pneumonia, or if symptoms do not quickly improve after starting antibiotic treatment, or if the patient is already in poor health, hospital admission may be advised.
A chest X-ray may be taken to confirm the diagnosis and the extent of the infection.
Blood tests and sputum tests may be taken to find which bacterium is causing the pneumonia. This helps to decide which antibiotic is best to use. Sometimes the bacterium that is causing the pneumonia is 'resistant' to the first antibiotic. A switch to another antibiotic is sometimes needed.
Sometimes oxygen and other supportive treatments are also needed.
Prevention of pneumonia
Do not smoke. Cigarette smoke damages the lining of the airways and makes the lungs more prone to infection.
Immunization.
Pneumococcal immunization. The pneumoccocus is a common cause of bacterial pneumonia.
Influenza immunization.
Pulmonary Tuberculosis
Tuberculosis (TB) is a common contagious disease caused by bacterium called Mycobacterium tuberculosis. Tuberculosis most commonly (75%) attacks the lungs (as pulmonary TB). In the other 25% of active cases, the infection moves from the lungs, causing other kinds of TB - the central nervous system, the cardiovascular system, the urinary / reproductive system, bones, joints and even the skin. If not treated properly, TB can be deadly.
Like the common cold, it spreads from person to person through the air. Only people who are sick with TB in their lungs can infect other people. When people with TB cough, sneeze, talk or spit, they propel TB germs into the air. People who are nearby can then possibly breathe the bacteria into their lungs. A person needs only to inhale a small number of these to be infected.
Left untreated, each person with active TB disease will infect on average between 10 and 15 people every year. But people infected with TB bacteria will not necessarily become sick with the disease. The immune system "walls off" the TB bacteria. However, the bacteria protected by a thick waxy coat, can live for years without causing any disease symptoms; when someone's immune system is weakened, the chances of becoming sick with TB are greater.
The following people are at higher risk for active TB:
Elderly
Infants
Persons with weakened immune systems, for example due to AIDS, chemotherapy.
Disseminated TB occurs when the infection invades the blood stream resulting in lesions which have the appearance of millet seeds on X-ray.
Facts about tuberculosis
· Someone in the world is newly infected with TB bacteria every second
· Overall, one-third of the world's population is currently infected with the TB bacteria
· Not everyone infected develops the full-blown disease; asymptomatic, latent TB infection is most common. However, one in ten latent infections will progress to active TB disease, which, if left untreated, kills more than half of its victims
· 5-10% of people who are infected with TB bacteria (but who are not infected with HIV) become sick or infectious at some time during their life. People with HIV and TB infection are much more likely to develop TB.
Local symptoms of pulmonary TB
· A bad phlegm producing cough that lasts 3 weeks or longer
· Chest pain
· Coughing up blood or mucus
Systemic symptoms of pulmonary TB
· Fever, chills
· Night sweats
· Appetite loss
· Weight loss
· Pallor
· Weakness or fatigue
Examinations and Tests
Examination of the lungs by stethoscope can reveal crackles (unusual breath sounds). Enlarged or tender lymph nodes may be present in the neck or other areas. Fluid may be detectable around a lung. Clubbing of the fingers or toes may be present.
Tests may include:
Chest x-ray
Sputum cultures
Tuberculin skin test
Chest CT
Treatment
The goal of treatment is to cure the infection with drugs that fight the tuberculosis bacteria. The initial treatment may involve a combination of many drugs. It is continued until laboratory tests show which medicine works best.
Treatment usually lasts for 6 months, but longer courses may be needed for persons with AIDS or whose disease responds slowly.
Symptoms may improve in 2 to 3 weeks; however, a chest x-ray will not show this improvement until later. Prognosis is excellent if pulmonary TB is diagnosed early and treatment is begun.
Patient may need to be admitted to a hospital to prevent the spread of the disease to others until no longer contagious.
Incomplete treatment of TB infections (such as failure to take medications for the prescribed length of time) can contribute to the emergence of drug-resistant strains of bacteria.
Prevention
TB is a preventable disease, even in those who have been exposed to an infected person. Skin testing (PPD) for TB is used in high risk populations or in individuals who may have been exposed to TB, such as health care workers.
A positive skin test indicates prior TB exposure. Individuals exposed to tuberculosis should be skin tested immediately and a follow-up test should be done at a later date, if the initial test is negative.
Prompt treatment is extremely important in controlling the spread of tuberculosis for those who have already progressed to active TB disease.
A BCG vaccination to prevent TB is given. People who have had BCG may still be skin tested for TB and results of testing (if positive) discussed with one's doctor.
Important things about tuberculosis to tell patients
TB is not usually caught by simply sitting next to an infected person. The infection requires prolonged and close contact in order to spread from person to person.
You do not get TB by just touching the clothes or shaking the hands of someone who is infected.
Your risk of contracting TB increases if you:
Are in frequent contact with people who have the disease
Live in crowded or unsanitary living conditions
Have poor nutrition
TB affects children and adults differently. It is very uncommon to catch TB from a child with the disease.
Symptoms include: fever and night sweats, persistent cough, weight loss and blood in sputum.
TB is curable. It is usually treated with a six-month course of antibiotics, which MUST be completed in order to discourage recurrence of disease or drug resistance.
Acute Respiratory Infections
Acute respiratory infections (ARI) are a leading cause of illness and death in children under age five in developing countries including Pakistan. They are caused by bacteria and viruses; often the viruses start the acute illness, followed by a superinfection caused by the bacteria. However, certain of the viruses may alone be responsible for life-threatening illness.
ARI is classified based on the site of infection as Acute Upper Respiratory Infections (AURI) and Acute Lower Respiratory Infections (ALRI).
AURI are very common in childhood. Though mostly self limiting, they are a leading cause of morbidity like deafness and learning handicaps. Examples of AURI include common cold, sore throat, tonsillitis, sinusitis and otitis media.
Important examples of ALRI include bronchitis and pneumonia. A large number of deaths in children under 5 years are due to ALRIs with 90% of these deaths being due to pneumonia.
Upper Respiratory Tract
· Common cold
o Main features include large amounts of watery to mucoid, sometimes purulent nasal discharge. It is sometimes accompanied by fever.
· Sore throat
o Generalized redness of throat, not localized to the tonsils. Some fever may be present.
· Tonsillitis
o Local infection of tonsils which are red and swollen with secretions on the surface.
· Sinusitis and Otitis Media
o Painful inflammatory conditions of sinuses and middle ear.
· Influenza
o Fever, muscle aches, sore throat, headache - usually not much nasal discharge compared to a cold. Maybe some cough.
Lower Respiratory Tract
· Acute Bronchitis
Inflammation of bronchi, accompanied by fever, cough, wheezing and "noisy chest".
· Pneumonia
See the section on Pneumonia
· Management of Acute Respiratory Infections
In the majority of cases the illness is due to viral infection and requires supportive measures only. The sick person should be provided with increased oral fluids to prevent dehydration, continued feeding (in case of children frequent breastfeeding to avoid malnutrition), analgesics for pain relief and anti-pyretics to reduce high fever. If the infection is considered to be bacterial and, if necessary, appropriate antibiotics should be given.
Lesson 4: Practical
· Vital health statistics: respiratory rate
Definition
The number of breaths taken per minute.
Measurement and recording of respiratory rate
The respiration rate is usually measured when a person is at rest.
Step 1:
Observe patient’s stomach or chest and watch until you see it rise and fall. Each rise/fall cycle counts as one respiration.
Step 2:
Count the number of times the stomach or chest rises for 30 seconds and multiply by 2, or count for a full 1 minute. This tells you the respiratory rate per minute.
Step 3:
Note the rhythm of the breathing. Is it regular or irregular?
Step 4:
Note how much effort it takes for the person to breathe. Is the breath labored, or effortless?
Step 5:
Note if the breathing is deep (slow) or shallow (fast).
Step 6:
Smell the breath for any unusual odor, especially noting a fruity odor or a fecal odor.
Step 7:
Record your findings in the following manner: rate, rhythm, effort, depth, noise and odors. For example: "Respiratory rate is 30, irregular, labored, shallow, gurgling and with no odor."
Average respiratory rates, by age
Newborns: Average 44 breaths per minute
Infants: 20-40 breaths per minute
Small children: 20-30 breaths per minute
Older children: 16-25 breaths per minute
Adults: 12 to 20 breaths per minute
Adults during strenuous exercise 35-45 breaths per minute
Athletes' peak 60-70 breaths per minute
Causes of increased respiratory rate
Respiration rates may increase with exercise, excitement, pain, fever, and with other medical conditions.
Causes of decreased respiratory rate
Respiration rates decline during relaxation and sleep.
Class room evaluation
Student: _________________________ ID:__________________________
Teacher: _________________________ Unit: Human body
Sub-unit 2.3 Date: ________________________
Inhaled oxygen molecules enters through the walls of the ___________ in the lungs. (choose one from the following)
a. artery
b. alveoli
c. arterioles
Right and left pulmonary arteries carry (choose one from the following)
a. oxygen-poor blood
b. oxygen-rich blood
c. oxygen-neutral blood
Newly oxygenated blood enters the heart through the pulmonary (choose one from the following)
a. artery
b. bronchus
c. vein.
Deoxygenated blood is taken from the heart to the lungs via the (choose one from the following)
a. aorta
b. inferior vena cava
c. pulmonary artery
From the lungs, high-oxygen blood moves through tiny blood vessels leading to the ____ where it is pumped to the rest of the body.
In the alveoli, oxygen is moved from the lungs into the blood, and ____ is moved from the blood into the lungs. (choose one from the following)
a. calcium phosphate
b. carbon dioxide
c. nitrous oxide
_____ travel single file through the capillaries so that materials can be diffused into or out of the circulatory system (choose one from the following).
a. glucose molecules
b. white blood cells
c. red blood cells
Capillaries associated with the alveoli, allow for the exchange of oxygen and carbon dioxide gases in the (choose one from the following)
a. blood platelet cells
b. red blood cells
c. white blood cells
Oxygenated blood from the ____ flows to the heart to be pumped to the body cells. (choose one from the following)
a. brain
b. lungs
c. kidneys
What gas is exhaled out? (choose one from the following)
a. carbon dioxide
b. sodium
c. oxygen
During breathing, the ____ will expand as it fills with gas and will become smaller as the gas leaves. (choose one from the following)
a. alveolus
b. capillary
c. larynx
The science term for the voice box is the
a. esophagus
b. larynx
c. pharynx
Signs and symptoms of pneumonia include (fill in the blanks using the clues given in the bracket
______ body temperature that may be accompanied by shaking chills (high, low)
______ respiratory rate (increased, decreased)
______ blood pressure (high, low)
______ heart rate (fast, slow)
Notes
Notes
Sub-unit 2.4
The Musculoskeletal System & Skin
Learning objectives:
After completing sub-unit 2.4 dispenser students will be able to:
a. demonstrate basic understanding of the musculoskeletal system and skin (What is the Musculoskeletal System? What comprises the system? What are the major functions of the system? What are the functions of its component parts?)
b. mark location of major parts of the system on human body, e.g. long bones of the body, origin/insertion of muscles of limbs and large joints
c. identify signs and symptoms of fractures and concerned vessel injuries
d. carry out immediate (emergency) management of fractures
e. develop a general understanding of anatomy and physiology of skin and recognize skin ailments such as scabies.
Introduction
Bones, muscles, and joints - along with tendons, ligaments, and cartilage - form the musculoskeletal system and enable us to do everyday physical activities. In this sub-unit we will focus on bones, muscles, and joints.
Lesson 1: Anatomy of the Musculoskeletal System
Activity
Ask students if they have ever seen bones, muscles, and joints of a goat or cow. If they remember seeing any of these, ask them to describe their gross features.
Bones
The skeleton or skeletal system is a strong framework that supports the body. A typical adult human skeleton is made of 206 bones, though this number varies owing to anatomical variations; for example, some people have an extra rib or an extra vertebra. The longest and heaviest bone in the body is the femur, and the smallest is the stapes bone in the middle ear. The skeleton holds the body erect, but not fixed in one position.
Bones begin to develop before birth. When the skeleton first forms, it is made of flexible cartilage, but within a few weeks the cartilage starts to get replaced by hard deposits of calcium phosphate and collagen, the two main components of bone. It takes about 20 years for this process to be completed.
The human skeleton can be divided into the axial skeleton and the appendicular skeleton:
The axial skeleton consists of the 80 bones in the head and trunk of the human body. The purpose of the axial skeleton (among other things) is to protect the body's most vital organs. It is composed of five parts:
· Skull
· Bones of the inner ear
· Hyoid bone of the throat
· Chest
· Vertebral column.
Figure 1: Axial skeleton
The appendicular skeleton consists of 126 bones which make movement possible and protects the organs of digestion, urination, and reproduction. It is composed of six parts:
Shoulder girdle
Arm
Hand
Pelvic girdle
Leg
Foot.
Figure 2: Appendicular skeleton
Figure 3: Major bones of the skeleton (front view)
Figure 4: Major bones of the skeleton (back view)
Types of bones
The skeleton is made up of bones that can be categorized according to one of four functions that they perform:
Long bones form the levers for movement of the arms (humerus, ulna, radius) and legs (femur, tibia, fibula). Other long bones are in the hands and the feet (metacarpals and metatarsals).
Flat bones provide protection to the vulnerable organs of the body. e.g. skull protects brain.
Short bones provide weight bearing and intricate movement. e.g. the carpals and tarsals (wrist and ankle).
Irregular bones provide shape and some protection. e.g. the bones of the face and the vertebrae.
Major long bones of the limbs
Upper limb
The humerus is a long bone in the arm that runs from the shoulder to the elbow.
The ulna (elbow bone) is placed at the little finger side of the forearm, parallel with the radius.
The radius is the bone of the forearm that extends from the elbow to the thumb side of the wrist.
Figure 5: Major long bones of the upper limb
Lower limb
The femur or thigh bone is the longest, most voluminous, and strongest bone. The average human femur is 48 centimeters in length and 2.34 cm in diameter and can support up to 30 times the weight of an adult.
The tibia or shinbone is the larger of the two leg bones below the knee. It is found on the big toe side of the leg. It is the second-longest bone in the human body.
The fibula or calf bone is the smaller of the two bones of the leg, and, in proportion to its length, the most slender of all the long bones.
Figure 6: Long bones of the lower limb
Muscles
Muscle is a tissue that can contract and cause motion. Muscles account for about half a person’s weight.
There are three types of muscle: (Add flexion & extension) & compartments
· Skeletal muscle or "voluntary muscle" is the type of muscle that we can see and feel. When a body builder works out to increase muscle mass, skeletal muscle is what is being exercised. It is also called ‘voluntary muscle’ because it usually contracts voluntarily, meaning that you think about contracting it and your nervous system tells it to do so. It is attached by tendons to bone mostly in the legs, arms, abdomen, chest, neck, and face. Voluntary muscles come in pairs - one muscle to move the bone in one direction and another to move it back the other way. These muscles hold the skeleton together, give the body shape, and help it with everyday movements.
Smooth muscle or "involuntary muscle" unlike skeletal muscle is not under our voluntary control; rather, they are controlled by the nervous system automatically. Smooth muscle is found in the digestive system, blood vessels, bladder, airways and, in a female, the uterus. Smooth muscle has the ability to stretch and maintain tension for long periods of time. It contracts involuntarily, meaning that you do not have to think about contracting it because your nervous system controls it automatically. For example, your stomach and intestines do their muscular thing all day long, and, for the most part, you never know what is going on in the gastrointestinal tract.
Cardiac muscle is also an "involuntary muscle" but is more similar in structure to skeletal muscle, and is found only in the heart. The walls of the heart's chambers are composed almost entirely of muscle fibers. Its rhythmic, powerful contractions force blood out of the heart as it beats.
Figure 7: Types of muscles – skeletal, smooth and cardiac
Figure 8 Skeletal muscles
Activity
Discuss what are the skeletal, smooth and cardiac muscles?
Joints
Activity
In small groups discuss the location of various joints of the body.
Name of movements
A joint is the location at which two or more bones make contact.
The joints may be classified anatomically into the following groups:
hand joints
wrist joint
elbow joint
axillary joint
sternoclavicular joint
vertebral joint
temporomandibular joint
sacroiliac joint
hip joint
knee joint
foot joints
Lesson 2: Physiology of the Musculoskeletal System
Bones
Activity
Brainstorm the main functions of the bony skeleton.
The bony skeleton has the following main functions:
· Shape and support
The skeleton provides the framework which supports the body and maintains its shape.
· Movement
Most of the bones are connected to other bones at flexible joints, which lend the skeleton a high degree of flexibility / movement. The bones provide attachment for the skeletal muscles and the ligaments of the joints. They then act as levers and pulleys translating the contraction of the skeletal muscles into movement.
· Protection
The skeleton provides protection for the body’s vital organs i.e. the brain, the eyes, and the middle and inner ears, spinal cord, lungs, heart, digestive, urinary and reproductive systems.
· Blood cell production
Red blood cells and some white blood cells are manufactured by the bone marrow which is found in the cavities of some of the larger bones.
· Storage
Bones store calcium and iron.
Muscles
The basic action of any muscle is contraction. Its function is to produce force and cause motion, either locomotion (voluntary movement) or movement within internal organs (involuntary movement). Much of muscle contraction is involuntary (it occurs without conscious thought) and is necessary for survival, like the contraction of the heart or peristalsis, which pushes food through the digestive system.
Voluntary muscle contraction is used to move the body. For example, when you think about moving your arm using your biceps muscle, your brain sends a signal down a nerve cell telling your biceps muscle to contract. The amount of force that the muscle creates varies - the muscle can contract a little or a lot depending on the signal that the nerve sends. Voluntary muscle contraction can produce fine movements like movements of fingers to button your shirt, or gross movements like the contraction of quadriceps muscle of the thigh resulting in straightening of knee joint. Cardiac muscle which is a type of involuntary muscle is concerned with the contraction of the heart - a movement which happens throughout each person’s life.
Activity
Discuss other examples of voluntary and involuntary movements.
Joints
Joints are constructed to allow movement and provide mechanical support. Joints can be classified by their range of movement as follows:
· Immovable (fixed) joints do not move. The dome of the skull, for example, is made of bones, which must be immovable to protect the brain. Between the bones are immovable joints. Other example is of the joints between the teeth and the jawbone.
· Partially movable joints move a little. They are found in the vertebral column. Each of the vertebrae moves in relation to the one above and below it, and together these movements give the vertebral column its flexibility.
· Freely movable joints move in many directions. The main joints of the body - found at the hip, shoulders, elbows, knees, wrists, and ankles - are freely movable. They are filled with a special fluid, which acts as a lubricant to help the joints move easily. There are three kinds of freely movable joints that play a big part in voluntary movement:
o Hinge joints allow movement in one direction, as seen in the knees and elbows.
o Pivot joints allow a rotating or twisting motion, like that of the head moving from side to side.
o Ball-and-socket joints allow the greatest freedom of movement. The hips and shoulders have this type of joint, in which the round end of a long bone fits into the hollow of another bone.
Activity
Move your knee, elbow, hips and shoulder joints and note what movements result from moving them. Compare your notes with your friends’ notes.
Also name the movements
Figure 9: Common types of joints
Activity
Brainstorm:
Why the shoulder and hip joints are of the ball and socket type?
Why the skull joints are of the fixed type?
Lesson 3: Disease states
Fractures
A fracture occurs when a bone breaks. If a fractured bone is to resume its normal function, it must be repaired. Bones are natural healers; at the location of the fracture, bones produce many new cells and tiny blood vessels that rebuild the bone. Fragments of broken bone are removed from the site by specialized bone cells, i.e. osteoclsts and another kind of cells osteoblasts produce new bone. Then another kind of special bone cells activate to produce new material which “knits” the ends of the bone together. Most fractures repair themselves within six weeks. Some bones, however, have a poor blood supply and repair takes longer. These include the neck of the femur and the lower portion of the tibia.
One of the most important influences on fracture healing is nutrition. The healing time for broken bones is influenced by a number of variables that are impacted by the availability of key nutrients to support bone healing and a healthy blood supply. As a fracture heals, it may be helpful to take a bone health supplement in order to ensure availability of key nutrients and provide for extra nutritional support during the healing process.
Signs and symptoms of a fracture
· A snap or a grinding noise is heard during the injury
· There is swelling, bruising, or tenderness around the injured part
· It is painful to bear weight on the injury, touch it, press on it, or move it
· The injured part looks deformed. In severe breaks, the broken bone may be protruding through the skin
· Immediate things you should do when managing a patient with a fracture
· Do not move the patient if
o the patient may have seriously injured the head, neck, or back
o the broken bone comes through the skin. Apply constant pressure with a clean gauze pad or thick cloth, and keep the patient lying down until help arrives. Do not wash the wound or push in any part of the bone that is sticking out.
· For less serious injuries, try to stabilize the injury as soon as it happens by following these quick steps
o Remove clothing from the injured part. Do not force a limb out of the clothing, though. You may need to cut clothing off with scissors to prevent causing the patient any unnecessary additional pain
o Apply a cold compress or ice pack wrapped in cloth
o Place a makeshift splint on the injured part by:
o keeping the injured limb in the position you find it
o placing soft padding around the injured part
o placing something firm (like a board or rolled-up newspapers) next to the injured part, making sure it is long enough to go past the joints above and below the injury
o keeping the splint in place with first-aid tape
o Do not allow the patient to eat, in case surgery is needed
Activity
Role Play
Ask students to form pairs.
Students act out the role of a dispenser and a person who has come with a closed fractured femur. Dispenser to carry out the immediate management of the fractured bone using the materials provided.
Reverse the role
Different types of fractures
Children's bones are more likely to bend than break completely because they are softer. Fracture types that are more common in children include:
buckle fracture: one side of the bone bends, raising a little buckle, without breaking the other side
greenstick fracture: a fracture in which one side of the bone is broken and the other side bends (like when trying to bend a living stick on a tree)
Mature bones are more likely to break completely. A stronger force will also result in a complete fracture of younger bones. A complete fracture may be a:
closed fracture: a fracture that does not break the skin
open (or compound) fracture: a fracture in which the ends of the broken bone break through the skin (these fractures have an increased risk of infection)
non-displaced fracture: a fracture in which the pieces on either side of the break line up
displaced fracture: a fracture in which the pieces on either side of the break are out of line (which might require surgery to make sure the bones are properly aligned before casting)
Other common fracture terms include:
hairline fracture: a thin break in the bone
single fracture: the bone is broken in one place
segmental: the bone is broken in two or more places in the same bone
First Aid Management
A splint is all that may be needed to keep the bone from moving so it can heal. A splint usually supports the broken bone on one side and might be needed to readjust later.
When a splint is applied, the following steps are undertaken:
· A layer of cotton is put first.
· Next, the splint is placed over the cotton. A splint may be made of stiff pieces of plastic or metal or can be molded out of plaster or fiberglass to fit the injured area comfortably.
· Then cloth or straps (which usually have Velcro) are used to keep the splint in place.
· Once the cast is on, the patient should prop the splinted area on a pillow for a few days to reduce swelling.
However, most broken bones will need a cast. A cast, which keeps a bone from moving so it can heal, encircles the entire broken area and is removed when the bone is healed. It is essentially a big bandage that has two layers — a soft cotton layer that rests against the skin and a hard outer layer that prevents the broken bone from moving.
Casts are made of either:
plaster of Paris: a heavy white powder that forms a thick paste that hardens quickly when mixed with water. Plaster of Paris casts are heavier than fiberglass casts and do not hold up as well in water.
synthetic (fiberglass) material: made out of fiberglass - a kind of moldable plastic - these casts come in many bright colors and are lighter and cooler. The covering (fiberglass) on synthetic casts is water-resistant, but the padding underneath is not.
When a cast is put on, the following steps are undertaken:
First, several layers of soft cotton are wrapped around the injured area.
Next, the plaster or fiberglass outer layer is soaked in water. The doctor wraps the plaster or fiberglass around the soft first layer. The outer layer is wet but will dry to a hard, protective covering. Doctors sometimes make tiny cuts in the sides of a cast to allow room for swelling.
Once the cast is on, the patient should prop the casted area on a pillow for a few days to reduce swelling.
Some pain is expected for the first few days after getting a cast, but it usually is not severe. The doctor may recommend paracetamol or ibuprofen.
If the cast is causing the patient’s fingers or toes to turn white, purple, or blue, the cast may be too tight and may need to be adjusted. Check for relevant pulse to determine the flow of blood in that area. Also if the skin around the edges of the cast gets red or raw — that is typically a sign that the cast is wet inside from sweat or water and may need to be adjusted.
If the cast or splint is on an arm, the patient may need a sling to help support it. A sling is made of cloth and a strap that loops around the back of the neck and acts like a special sleeve to keep the arm comfortable and in place. A patient with a broken leg will probably get crutches to make it a little easier to get around.
· Closed reduction
For displaced fractures (in which the pieces on either side of the break are out of line), the bone will need to be set before putting on a cast. To set the bone, the doctor will put the pieces of the broken bone in the right position so they can grow back together into one bone (this is called a closed reduction). During a closed reduction, the doctor will realign the broken bone so that it heals in a straighter position. The patient is given medicine when this is done to help keep the bone from hurting. A cast is then put on to keep the bone in position.
· Surgery
Although most broken bones simply need a cast to heal, other more serious fractures (such as compound fractures) may require surgery to be properly aligned and to ensure the bones stay together during the healing process. Open fractures need to be cleaned thoroughly in the sterile environment of the operating room before they are set because the bone's exposure to the air poses a risk of infection.
With breaks in larger bones or when the bone breaks into more than two pieces, the doctor may put a metal pin in the bone to help set it before placing a cast. When the bone has healed, the doctor will remove the pin.
How can the risk for fractures be minimised?
A healthy diet, high in vitamins and minerals will help keep bones strong. In addition to proper nutrition, weight bearing exercise e.g. walking will help keep bones strong and improve balance and coordination. The consequences of falls can be death, injuries, fractures, hospitalisation, and permanent disability. The three most predictive factors for falling are muscle weakness around the hip joint, increased unsteadiness and intake of more than three medications.Tips for people to avoid fracture risk
• Engage in walking or other weight bearing activities to improve both muscle and bone. Exercise also improves balance and coordination.
• Make sure your stairways and hallways at home have bright lights.
• Maintain a healthy diet with lots of vitamins and minerals, especially calcium and vitamin D.
• Eliminate all tripping hazards at home, such as loose rugs; repair any loose carpeting or floorboards.
• Remove loose electrical cords.
• Use sturdy hand rails when walking down steps.
• Provide enough light to see each step at both the top and bottom of stairways.
• Arrange household furniture in ways that provide plenty of walking room.
• Install slip resistant strips on floor of shower.
• Wear properly fitting shoes with nonskid soles; tie shoelaces.
• In the kitchen, place a rubber mat in front of your sink so you will not slip on water.
• Store items on shelves and in cabinets that are at waist level. Avoid reaching for things that are too high.
Lesson 4: Practical
Activity
In pairs and with the help of a chalk, mark the location of humerus, radius, ulna, femur, tibia and fibula on your friend’s body.
Once done, have a look at Figure 9 to see if the marking has been done correctly.
Figure 10: The skeleton
Activity
On the handout given to you, you will find drawings of a disarticulated skeleton. This skeleton is all mixed up and needs your help to be put together again. Cut out the pieces and ‘reassemble’ the skeleton onto a piece of paper without the aid of a picture of an entire skeleton. Before you glue down your pieces, check your arrangement against the skeleton drawing in your book. After correctly gluing the skeleton to the paper, label the names of all the bones you can.
Handout
Students should be provided with a handout of a disarticulated skeleton (attached). Click here to open handout (PDF Document)
Lesson 5: Skin
Activity
Brainstorming: Ask students about what they understand of the structure of skin? What are its functions? What is the importance of skin to healthcare workers?
Anatomy
Skin is the largest and a vital organ in the human body. It covers the entire external surface of the human body and is the principal site of interaction with the surrounding environment. It serves as a protective barrier preventing internal tissues from exposure to trauma, ultraviolet radiation, temperature extremes, toxins, and bacteria. Other important functions include sensory perception, immunologic surveillance, temperature-regulation, and control of insensible fluid loss. It keeps the inside of our body inside, and keeps what's outside of our body outside. Skin also helps maintain a constant body temperature. It is only about 0.07 inches (2 mm) thick.
Skin is made up of two layers. The outer layer is called the epidermis; it is a tough protective layer that contains melanin (which protects against the rays of the sun and gives the skin its color).
The second layer (located under the epidermis) is called the dermis; it contains nerve endings, sweat glands, oil glands, and hair follicles.
Under these two skin layers is the third fatty layer of subcutaneous tissue (the word subcutaneous means "under the skin").
On average, an adult has up to 2 square meters of skin, which weighs between 4.5 to 5 kilograms.
Figure 11
Structures in the Skin:
Figure 11 shows a cross section of skin
Blood vessels: Tubes that carry blood as it circulates. Arteries bring oxygenated blood from the heart and lungs; veins return oxygen-depleted blood back to the heart and lungs. In conditions such as pneumonia and congestive heart failure, the oxygenation of blood is compromised. Oxygen depleted blood in these conditions gives a bluish color to the skin which is called cyanosis.
Dermis: (also called the cutis) the layer of the skin just beneath the epidermis.
Epidermis: the outer layer of the skin.
Hair follicle: a tube-shaped sheath that surrounds the part of the hair that is under the skin. It is located in the epidermis and the dermis. The hair is nourished by the follicle at its base (this is also where the hair grows).
Hair shaft: The part of the hair that is above the skin.
Hair erector muscle: a muscle is connected to each hair follicle and the skin - it contracts (in response to cold, fear, etc.), resulting in an erect hair and a "goosebump" on the skin.
Melanocyte: a cell in the epidermis that produces melanin (a dark-colored pigment that protects the skin from sunlight).Pacinian corpuscle: - nerve receptors that respond to pressure and vibration; they are oval capsules of sensory nerve fibers located in the subcutaneous fatty tissueSebaceous gland: a small, sack-shaped gland that releases oily (fatty) liquids onto the hair follicle (the oil lubricated and softens the skin). These glands are located in the dermis, usually next to hair follicles.Sweat gland: (also called sudoriferous gland) a tube-shaped gland that produces perspiration (sweat). The gland is located in the epidermis; it releases sweat onto the skin.Subcutaneous tissue: fatty tissue located under the dermis.
Functions of Skin
The skin has very important vital functions for keeping the physiological and biochemical conditions of the body in its optimum state. The most important functions of the skin are:
· Regulates body temperature.
· Prevents loss of essential body fluids, and penetration of toxic substances.
· Protection of the body from harmful effects of the sun and radiation.
· Excretes toxic substances with sweat.
· Mechanical support.
· Immunological function mediated by Langerhans cells.
· Sensory organ for touch, heat, cold and emotional sensations.
· Vitamin D synthesis from its precursors under the effect of sunlight and introversion of steroids.
The epidermis is the outer most layer of skin that acts as a barrier preventing toxic chemical and other materials from penetrating deeper into the skin. This is relatively porous and undergoes changes in thickness in response to different factors such as trauma or pressure.
The layers of the epidermis differentiate and gradually develop to a more rigid structure, which provides a barrier to excessive loss of body fluids and the penetration of noxious substances. The basal layer is the precursor of the different cells of the epidermis which divide, pushed further upwards, loosing much of their metabolic function and enzymatic activity. The spinous layer is characterized by growth of keratin fibrils where these are present also in the cells of the basal layer.
Epidermal cells as they are pushed up away from the basal layer, begin to dehydrate and become filled with cross-linked keratin, which gives the cells a granular appearance. Lamellar bodies containing lipids play an important role in skin protection. The intercellular lipids, the corneocytes, amino acids, and other salts from sweat, sebaceous secretions, degradation products from corneal proteins besides lipids and others all have an important barrier effect preventing loss of water and keep the skin pH in its optimum condition (5.5).
The stratum corneum provides most of the barrier function.
The skin acts as a two-way barrier to prevent the inward or outward passage of water and electrolytes. The epidermis largely represents the barrier; whereas once the epidermis is removed the residual dermis is almost completely permeable.
Common Skin Disorders
There are more than a thousand conditions that may affect the skin but most skin diseases can be categorized according to nine common types.
Rashes
A rash is an area of red, inflamed skin or a group a individual spots. These can be caused by irritation, allergy, infection an underlying disease, as well as by structural defects - for example blocked pores or malfunctioning oil glands. Examples of rashes dude acne, dermatitis, eczema, hives, pityriasis rosea, and psorasis.
Viral infections:
These occur when a virus penetrates the stratum corneum and infects the inner layers of the skin. Example viral skin infections include herpes simplex, shingles (herpes zoster) and warts. Some systemic viral infections, such as chicken pox at measles, may also affect the skin. Viral infections cannot be cured with antibiotics.
Bacterial infections:
Such infections are caused by a variety of bacteria, the most common types being staphylococci streptococci. Bacteria may infect the topmost layers of skin, the follicles, or the deeper layers of skin. If not treated correctly, these infections may spread throughout the body. Examples include impel folliculitis, cellulitis, and Lyme disease. Antibiotics are effective against bacterial infections.
Fungal infections:
Harmless fungi are always present on surface of the skin, and infection occurs when these organisms entry into the body These infections are usually superficial, affecting the skin, hair, and nails; examples include athlete’s foot, lock itch, and ringworm. However, in people with suppressed immune systems or who have been taking antibiotics long-term, the fungi may spread to deep within the body, causing more serious disease.
Parasitic infections:
These infections occur after exposure to parasites such as lice and scabies.
Scabies
Scabies is a skin condition caused by a tiny mite. It is quite common in Pakistan. It usually causes a typical itchy rash. It can affect anyone of any age. It can be passed on to others by close skin-to-skin contact. Treatment with a cream or lotion will usually cure scabies, but you need to apply it properly to every part of your body. Two applications of treatment are needed, seven days apart.
Scabies mite is called Sarcoptes scabiei. Mites are small eight-legged parasites (in contrast to insects, which have six legs). They are tiny, just 1/3 millimeter long, and burrow into the skin to produce intense itching, which tends to be worse at night. The mites which cause scabies are not visible with the naked eye but can be seen with a magnifying glass or microscope (Figure 11).
How do you get scabies?
Close skin-to-skin contact with an infected person is needed to catch scabies. Most cases are probably caught from holding hands with an infected person. The hand is the most common site to be first affected. The skin-to-skin contact needs to be for a reasonable time to catch the mite. Therefore, we are unlikely to catch scabies from an infected person by casual short contact such as a handshake or a hug.
The mites live in skin but die after a short time if they are away from the skin. Therefore, we are unlikely to catch scabies from bedding, towels, etc, unless we use them immediately after being used by someone with scabies. However, to play safe, it is best to treat bedding, towels, etc, as described later on.
Sometimes outbreaks of scabies occur in nurseries, residential homes, etc, where people are in regular close contact.
What are the symptoms of scabies? (Figure 12)
Mite tunnels (burrows) may be seen on the skin as fine, dark, or silvery lines about 2-10 mm long. The most common areas where they occur are the loose skin between the fingers, the front of wrists, and the hands. However, they can occur on any part of the skin. We may not notice the burrows until a rash or itch develops.
Itch is often severe. Itch tends to be in one area at first (often the hands), and then spreads to other areas. The itch tends to be worse at night and after a hot bath.
A rash usually appears soon after the itch starts. It is typically a blotchy, lumpy red rash that can appear anywhere on the body. The rash is often most obvious on the inside of the thighs, parts of the abdomen and buttocks, armpits, and around the nipples in women. The look of the rash is often typical of scabies. However, some people develop unusual rashes which may be confused with other skin conditions.
Scratching sometimes causes slight skin damage. In some cases the damaged skin becomes infected by bacteria - a 'secondary' skin infection. If skin becomes infected with bacteria it becomes red, inflamed, hot, and tender.
Figure 12
Who should be treated?
Scabies will persist indefinitely if not treated. Treatment is needed for:
Anybody who has scabies AND
All household members and close contacts of the affected person - even if they have no symptoms. This is because it can take up to six weeks to develop symptoms after you become infected. Close contacts may be infected, but have no symptoms, and may pass on the mite.
Note: everyone who is treated should be treated at the same time - that is, on the same day.
What is the treatment for scabies?
Scabies is curable. The usual treatment is with permethrin 5% dermal cream or .5% aqueous malathion lotion. Permethrin is an insecticide that kills the mites. Re-apply the same treatment seven days after the first application. This helps to make sure that all the mites are killed.
The following is a general guide about treatment which gives tips for success.
We need to treat all the skin of your body (including the back, soles of the feet, between fingers and toes, under fingernails, scalp, neck, face, ears, and genitals). Pay special attention to the areas where mite burrows most commonly occur. That is, the front of the wrists and elbows, beneath the breasts, the armpits, and around the nipples in women.
An adult needs at least 30g of cream or 100ml of lotion to cover the whole body. Apply cream or lotion to cool dry skin (not after a bath).
The cream or lotion should be left on for the full recommended time. This time can vary depending on which one you use. For example, it is 8-12 hours for permethrin cream and 24 hours for malathion lotion.
Children should stay off school until the first application of treatment has been completed.
If we wash our hands or any other part of our body during the treatment period, we should re-apply the cream or lotion to the washed areas.
Breastfeeding mothers should wash off the lotion or cream from the nipples before breastfeeding, and re-apply treatment after the feed.
Cover hands of babies with gloves or some other thing to stop them from licking the cream or lotion off their hands.
Clothes, towels, and bed linen should be machine washed with boiling hot water after the first application of treatment. This kills any mites that may be present. Keep any items of clothing that cannot be washed in plastic bags for at least 72 hours to contain the mites until they die. An alternative option to kill any mites on clothes and linen are: ironing the item with a hot iron, dry cleaning.
Some people who develop a secondary skin infection may also need antibiotics.
Common reasons why treatment fails, or for scabies to recur are:
the cream or lotion is not put on correctly for the full time, or
a close contact is not treated at the same time, and the infection is passed back.
Note: we will still be itchy for a while after successful treatment
It is normal to take up to 2-3 weeks (and sometimes up to six weeks) for the itch to go completely after the mites have been killed by treatment. Also, even after successful treatment, in a small number of cases there remain some itchy brownish red lumps (nodules) up to 2cm in diameter. If these remain they most commonly occur on the genitals and arm pits. These lumps are not infectious or mean that the mite is still present. They occur in some cases as a prolonged skin reaction to the scabies mite. If they occur they usually go within three months, but occasionally last up to one year.
Treatment for itch
While waiting for the itch to go after killing the mites, we may wish to try something to ease the itch. Options include the following:
Crotamiton cream or lotion has soothing qualities and may help to relieve itch. Apply crotamiton 2-3 times a day (but only once a day for children under three years old).
Hydrocortisone cream. This is a mild steroid cream that may ease any inflammation and help ease itch.
An antihistamine medicine that makes you drowsy such as chlorphenamine. This does not ease the itch directly, but can help you to sleep if itching is a problem at night (particularly for children).
Figure 13
Pigmentation disorders:
The amount of pigment in the skin is determined by the amount of melanin being produced by the body. Loss of pigment (hypo-pigmentation) can be caused by an absence of melanocytes, malfunctioning cells, exposure to cold or chemicals, or some types of infection. An increase in pigment (hyper-pigmentation) may be caused by skin irritation, hormonal changes, aging, a metabolic disorder, or another underlying problem. Age spots, freckles, and melasma are examples of hyper-pigmentation; vitiligo is an example of hypo-pigmentation.
Tumors and cancers:
These growths arise when skin cells begin to multiply faster than normal. Not every skin growth is cancerous: Some tumors are harmless and will not spread. Skin cancer is the most common of all the cancers. It is caused, in 90 percent of cases, by sun exposure. The three types of skin cancer are basal cell cancer (the most curable), squamous cell cancer (which may grow and spread), and malignant melanoma (the most deadly form). Prevention involves protecting the skin against damaging ultraviolet rays. Early detection helps to improve the chances of a cure, so regular self-examinations are recommended.
Trauma:
Trauma describes an injury to the skin caused by a blow, cut, or burn. Any time the surface of the skin is broken, the body becomes more susceptible to infection and disease.
Other conditions:
Wrinkles, rosacea, spider veins, and varicose veins are among those conditions that cannot be neatly categorized. Wrinkles are caused by a breakdown of the collagen and elastin within the dermis, which results in sagging skin. Rosacea is a long term disorder in which the skin of the face becomes red and develops pimples, lesions, and more rarely enlargement of the nose. Its cause is unknown. Spider veins and varicose veins become apparent when blood vessels enlarge and become visible through the surface of the skin.
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: Human body
Sub-unit 2.4 Date: ________________________
The following constitute the musculoskeletal system (circle the 3 correct answers)
a. Tendons
b. Nerves
c. Capillaries
d. Ligaments
e. Muscles
A typical adult human skeleton is made of _______ bones.
The axial skeleton consists of the ______ bones in the _____ and _____ of the human body.
Long bones include the following (circle the 4 correct answers)
a. Radius
b. Fibula
c. Vertebrae
d. Femur
e. Ulna
The __________ is the longest, most voluminous, and strongest bone in the body.
The three types of muscles in the body are
a. ______________ muscle
b. ______________ muscle
c. ______________ muscle
A joint is the location at which two or more _________ make contact.
The bony skeleton has the following main functions (circle the 3 correct answers)
a. exchange of oxygen and carbon dioxide
b. storage of calcium and iron
c. conduction of nerve impulses
d. protection for the body’s vital organs
e. production of blood cells
Some joints allow more _________________ than the others.
Describe the location of femur, tibia and fibula in the body.
________________________________________________________________________________________________________________________________________________________________________________________________________________________
Mark the bones in the following diagram
Notes
Notes
Sub-unit 2.5
The Nervous System
Learning objectives:
After completing sub-unit 2.5 dispenser students will be able to:
a. name major parts of the nervous system and describe their major functions
b. identify signs and symptoms of head injuries, spinal injuries and stroke
carry out immediate management (emergency) of head injuries, spinal injuries and stroke
The nervous system is a highly specialized network whose main components are cells called neurons. Neurons are interconnected to each other, and have the property of conducting, using electrochemical signals, a great variety of stimuli within the nervous system as well as from and towards most other systems.
Lesson 1: Anatomy of the Nervous System
Division of the Nervous System
Nervous system can be subdivided as follows:
· The central nervous system (CNS)
o Brain
o Spinal cord
· The peripheral nervous system (PNS)
o Sensory and somatic nervous system
§ Cranial nerves
§ Spinal nerves
o Autonomic nervous system
§ Sympathetic nervous system
§ Parasympathetic nervous system
Table 1: Division of the Nervous System
Nervous System
í
î
Central nervous system (CNS)
Peripheral nervous system (PNS)
í
î
í
î
Brain
Spinal cord
Sensory-somatic
nervous system
Autonomic
nervous system
í
î
í
î
Cranial nerves
Spinal nerves
Sympa-
thetic nervous system
Parasym-pathetic nervous system
The nervous system is a highly specialized network that is made of millions and millions of microscopic cells called neurons. The neurons are present in both the CNS and PNS and are the main type of brain cells. All neurons are shaped like flat stars and have long branches called dendrites coming off. Neurons are interconnected to each other through these branches. The junction between two neurons is called a synapse.
At birth, the brain has all the neurons it will ever have, but many of them are not connected to each other. When we learn things, the messages travel from one neuron to another, over and over. Eventually, the brain starts to create connections (or pathways) between the neurons, so things become easier and we can do them better and better.
Figure 1: Neurons with their long branches
Figure 2: Neurons showing dendrites and synapses
The Central Nervous System (CNS)
It is the larger part of the nervous system. It includes the brain and the spinal cord.
Brain
The brain lies within the skull (head bones). It is a soft wrinkled organ. It is made of more than 10 billion nerve cells and over 50 billion other cells and weighs about 1-1.5 kg. It is covered by the meninges (three-layered membranes that separate the skull from the brain) and is also protected by the skull. The brain is bathed in the cerebrospinal fluid (CSF), which circulates between layers of the meninges and through cavities in the brain. The CSF allows the brain to float and protects the nervous system. Brain has the following five parts:
i. Cerebrum: The biggest part of the brain is the cerebrum and makes up 85% of the brain's weight. The cerebrum has two halves, with one on either side of the head. The right half of the cerebrum controls the left side of the body, and the left half controls the right side of the body. The cerebrum is the thinking part of the brain, i.e. when we think, we use the cerebrum and our memory (both short-term and long-term) lives in the cerebrum. Cerebrum also controls the voluntary muscles — the muscles that move when we want them to.
Figure 3: Brain with cerebrum highlighted in purple color
Activity
Discuss some examples of short-term and long-term memory.
Discuss some examples of voluntary muscles.
ii. Cerebellum: The cerebellum is at the back of the brain, below the cerebrum. It is much smaller than the cerebrum but it is a very important part of the brain. Cerebellum controls balance, movement, and coordination (how muscles work together). Because of the cerebellum, one can stand upright, keep balance, and move around.
Figure 4: Brain with cerebellum highlighted in green color
iii. Brain stem: this is also a small part of the brain but performs many important functions. It sits below the cerebrum and in front of the cerebellum. It connects the rest of the brain to the spinal cord, which runs down the neck and back. The brain stem is in charge of all the functions the body needs to stay alive, like breathing air, digesting food, and circulating blood. It is the brain stem that tells the heart to pump more blood when during exercise or stomach to start digesting food. Part of the brain stem's job is to control the involuntary muscles — the ones that work automatically, without one even thinking about it.
Figure 5: Brain with brain stem highlighted in orange colour
Activity:
Discuss examples of involuntary muscles in the body.
What effect has the brain stem on these involuntary muscles?
iv. Pituitary gland: The pituitary gland is very small — only about the size of a pea. Its job is to produce and release hormones (see Unit 2, Sub-unit 2.8, Endocrine System).
Figure 6: Brain with pituitary gland highlighted in red color
v. Hypothalamus: Like pituitary gland, the hypothalamus is also an endocrine gland (see Unit 2, Sub-unit 2.8, Endocrine System).
Figure 7: Brain with hypothalamus highlighted in yellow color
Figure 8: Cerebrum
Spinal Cord
The spinal cord is a long, thin bundle of nerves. It is an extension of the central nervous system and is connected above to the brain. Below, it goes down the middle of the back and is surrounded and protected by the bony vertebral column. It is about 42-45 cm long and is about the diameter of a human finger. The three meninges that cover the brain are continuous with those covering the spinal cord separating spinal cord from the vertebral column. Like the brain, the spinal cord is also surrounded by the CSF that acts as a cushion to protect the delicate nerve against damage from banging against the inside of the vertebrae. It is the spinal cord and nerves that let messages flow back and forth between the brain and body.
Figure 9: Central nervous system showing brain and spinal cord
Figure 9
The peripheral nervous system (PNS)
It is the smaller part of the nervous system. It lies outside the CNS. It consists of millions of nerve fibers which connect the spinal cord to the arms, hands, legs and feet. There are two kinds of nerve in the PNS:
i. Motor nerves transmit impulses from the CNS to muscles and glands. These impulses activate muscles to contract (make body parts move) and glands to secrete
ii. Sensory nerves transmit impulses to the CNS from sensory receptors located throughout the body i.e. skin, skeletal muscles, joints and internal organs. They keep the CNS informed of events going on both inside and outside the body.
The peripheral nervous system It is subdivided into the:
Sensory-somatic nervous system
This consists of 12 pairs of cranial nerves which come directly out of the brain and carry impulses to and from the brain and 31 pairs of spinal nerves which come out of the spinal cord and carry impulses to and from the spinal cord.
Table 2: Twelve cranial nerves and their functions
Cranial Nerve
Major functions
I.
Olfactory
Transmits the sense of smell
II.
Optic
Transmits visual information
III.
Oculomotor
Performs most eye movements
IV.
Trochlear
Performs some eye movements (turns eyes downward and to the sides)
V.
Trigeminal
Performs chewing Receives sensation from the face
VI.
Abducens
Performs some eye movements (turns eyes to the sides)
VII.
Facial
Controls most facial expressions Responsible for secretion of tears and salivaTransmits sensation of taste
VIII.
Vestibulocochlear
Responsible for hearing Responsible for balance and movement sensation
IX.
Glossopharyngeal
Transmits sensation of taste
X.
Vagus
Slows heart rate Stimulates digestive organs
Controls muscles for voice
XI.
Accessory
Controls neck muscles
Controls swallowing movements
XII.
Hypoglossal
Controls tongue movements
Figure 10: Thirty one pairs of spinal nerves coming out of the spinal cord (number of spinal nerves)
Figure 10
Autonomic Nervous System (ANS):
The ANS performs "automatic" functions that we are seldom aware of. Autonomic nerves go from the spinal cord to the lungs, heart, stomach, intestines, bladder, and sex organs. It regulates the activity of smooth (involuntary) muscles, cardiac muscles, and glands. Examples are pumping of the heart and the release of hormones from the glands.
The ANS is further divided into the sympathetic nervous system and the parasympathetic nervous system. They generally serve the same organs but cause opposite effects. If one division stimulates certain smooth muscles to contract or a gland to secrete, the other division inhibits that action. This opposition is complementary in nature and not antagonistic. This opposition could be compared as the sympathetic division acting like the accelerator of a car and the parasympathetic division as its brake.
Sympathetic nervous system
The sympathetic nervous system is active when we are excited or are in emergency or threatening situations such as being frightened by a dog. It becomes more active during times of stress and promotes a "fight or flight" response.
Fight or flight response
· Heart rate is increased
· Respiratory rate is increased and respiration is deep
· Cold, sweaty skin (e.g. pale face) due to contraction of blood vessels
· Blood flow is directed away from the gastrointestinal tract (digestion is inhibited)
· Blood flow to skeletal (voluntary) muscles is increased
· Pupils are dilated and the lens relaxed, allowing more light to enter the eye
· Bladder is relaxed (urination)
· Inhibition of glands producing tears (dry eyes) and saliva (dry mouth)
Parasympathetic nervous system
The parasympathetic nervous system keeps body energy use as low as possible. It promotes a "rest and digest" response; promotes calming of the nerves and enhances digestion.
Functions of parasympathetic nervous system
· Increases blood flow of the gastrointestinal tract. This is important following the consumption of food
· Salivary gland secretion is stimulated, and peristalsis is accelerated
· Constriction of the eye pupil and lens.
Activity
In small groups discuss:
§ Examples of body activities which automatically take place and of which we are not usually aware. One example is the beating of the heart.
§ What sensations do sensory nerves carry from the skin?
§ What sensations do sensory nerves carry from the sensory organs?
§ When glands are stimulated by motor nerves, what secretions are produced?
§ What happens to a person when he/she is frightened or fighting or running away from someone?
Figure 11: Central and peripheral nervous systems
Figure 12: Different kinds of nerves
Lesson 2: Physiology of the nervous system
The nervous system is the control center for the entire body. The brain uses information it receives from the nerves to coordinate all of body actions and reactions. Nerves are the thin threads of neurons that run throughout the body. Bundled together, they carry messages back and forth just the way that telephone wires do. Sensory nerves send messages to the brain. Motor nerves carry messages back from the brain to all the muscles and glands in the body.
Nerves pass along message with the help of chemicals and electricity. When a neuron is stimulated - by heat, cold, touch, sound vibrations or some other message - it begins to generate a tiny electrical pulse. This pulse travels the full length of the neuron. But when it gets to the end of the neuron’s branch, it needs help getting across to the next branch. That is where chemicals (neurotransmitters) come in. The electrical pulse in the cells triggers the release of chemicals that carry the pulse to the next neuron. And so on and so on. A nerve cell can transmit 1,000 electrical impulses each second.
The fact that the nervous system uses a mixture of electrical and chemical signals makes it incredibly fast, which is necessary to acknowledge the presence of danger, for example, a hand touching fire. If the nervous system only comprised chemical signals, the body would not tell the arm to move fast enough to escape dangerous burns. So the speed of the nervous system is a necessity for life.
Different parts of the brain do different things. Some areas receive messages from sense organs, others control balance and muscle coordination, others handle speech, or emotion, memories, or basic motor skills, or complex calculations. One may think the heart is where you feel emotion, but it is really the brain. You may think your legs take you down the street, but it is the brain instructing the muscles in the legs to move. The eyes may take in light and an image may be projected onto the pupil, but it is the brain that interprets what one sees.
Tasting, smelling, seeing, hearing, thinking, dreaming, breathing, heart beating, moving, running, sleeping, laughing, singing, remembering, feeling pain or pleasure you could not do any of these things without your central nervous system. There is a very narrow gap between the neurons - the synaptic cleft, where an action potential is transmitted from one neuron to a neighboring one.
Lesson 3: Disease states
Head Injury
Definition
A head injury is a general term used to describe any trauma to the head that leads to injury of the scalp, skull, or brain. The injuries can range from a minor bump on the skull to serious brain injury. Head injury could result in a fracture, which is a break in the bone surrounding the brain and other structures within the skull. It could also result in intracranial (inside the skull) bleeding.
Head injury is classified as either closed or open (penetrating).
A closed head injury describes any injury to the brain or structures within the skull that is not caused by a penetrating injury (such as a gunshot wound or stab wound). The patient receives a hard blow to the head from striking an object. It ranges from very minor to potentially fatal injury.
An open, or penetrating, head injury means the patient was hit with an object that broke the skull and entered the brain. Bullets or sharp instruments (knives, screwdrivers, ice picks) may penetrate the skull. The initial injury itself may cause immediate death, especially if from a high-energy missile such as a bullet.
Concussion, the most common type of traumatic brain injury, is an injury to the brain that results from an impact to the head. It is not a life–threatening injury.
Contusion is a form of traumatic brain injury and is a bruise of the brain tissue. Small blood vessels leak into brain tissue and cause swelling of the brain. It is often caused by a blow to the head.
Causes
Common causes of head injury include:
§ Motor vehicle accidents
§ Falls (most common cause of head injury in children)
§ Physical assault, and
§ Accidents at home, work, outdoors, or while playing sports.
Signs and symptoms
Signs and symptoms of head injuries vary with the type and severity of the injury. The signs can occur immediately or develop slowly over several hours. Even if the skull is not fractured, the brain can bang against the inside of the skull and be bruised. The head may look fine, but complications could result from bleeding inside the skull.
Minor blunt head injuries may involve only symptoms of being "dazed" or brief loss of consciousness. They may result in headaches or blurring of vision or nausea and vomiting.
Severe blunt head injury involves a loss of consciousness lasting from several minutes to many days or longer. Fits may result. The person may suffer from severe and sometimes permanent neurological deficits or may die. Neurological deficits include paralysis, seizures, difficulty speaking, seeing, hearing, walking, or understanding.
Penetrating trauma may cause immediate, severe symptoms or only minor symptoms despite a potentially life-threatening injury. Death may follow from the initial injury. Any of the signs of serious blunt head trauma may result.
When managing a person who just had a head injury, try to find out what happened. If he or she cannot tell you, look for clues and ask witnesses. In any serious head trauma, always assume the spinal cord is also injured.
The following signs suggest a serious head injury and require emergency medical treatment:
· Loss of consciousness, confusion, or drowsiness
· Low breathing rate or drop in blood pressure
· Fits
· Fracture in the skull or face, facial bruising, swelling at the site of the injury, or scalp wound
· Fluid drainage from nose, mouth, or ears (may be clear or bloody)
· Severe headache
· Initial improvement followed by worsening symptoms
· Irritability (especially in children), personality changes, or unusual behavior
· Restlessness, clumsiness, lack of coordination
· Slurred speech or blurred vision
· Inability to move one or more limbs
· Stiff neck or vomiting
· Pupil changes
· Inability to hear, see, taste, or smell
Long-term effects of head injury
Some head injuries result in prolonged or non-reversible brain damage. This can occur as a result of bleeding inside the brain or forces that damage the brain directly. These more serious head injuries may cause:
Changes in personality, emotions, or mental abilities
Speech and language problems
Loss of sensation, hearing, vision, taste, or smell
Seizures
Paralysis
Coma
Diagnostic aids
History of the exact details of the injury, the person's past medical history, and the symptoms are often the most important information to make treatment decisions.
X-ray of skull is done in the following situations:
To look for a fracture in the skull bone. The presence of a skull fracture on x-ray does not mean there has been an injury to the brain, and the absence of a fracture does not exclude a brain injury. With or without a fracture, the most critical factor is determining if a brain injury is present. The fracture itself will seldom need treatment, but an underlying brain injury may. If the potential for a serious injury to the brain exists, a CT scan may be necessary.
In children younger than 1 year.
In people with a penetrating injury.
To locate foreign bodies and determine their number.
CT scan is the test used most often to evaluate acute head injuries. A CT scan is useful for identifying injuries to the brain itself. The CT is essentially an x-ray machine that takes multiple x-rays from many angles around the head. A computer uses these x-ray images to make a picture of the brain and other structures inside the skull. The picture is usually displayed as two-dimensional "slices" of various levels of the brain. The details on a CT scan are very good, and even small spots of blood may be seen as little white dots.
MRI scans are rarely used immediately after head injuries. The MRI may be used later for additional information about a brain injury.
In some cases of bleeding in or around the brain, angiography may be performed to visualize the blood vessels. This test involves injecting dye into the arteries of the head. X-rays are taken that show the blood vessels and may show exactly where bleeding is occurring. In some cases it is possible to stop the bleeding during angiography. This involves injecting special materials, which are released into the bleeding blood vessel and cause a clot to form. If this procedure is successful, the bleeding is stopped without the need for surgery.
Other x-rays may be performed to look for other illnesses or injuries. For example, neck injuries are common in people with severe head trauma. Spine x-rays are usually ordered before the head is moved if there is any neck pain or other symptoms of a neck injury. In a car accident, there may also be chest or abdominal injuries.
First Aid
Learning to recognize a serious head injury, and implementing basic first aid, can make the difference in saving someone's life. In patients who have suffered a severe head injury, there is often one or more other organ systems injured. For example, a head injury is sometimes accompanied by a spinal injury.
A doctor’s help is needed immediately if the person:
Becomes unusually drowsy
Develops a severe headache or stiff neck
Vomits more than once
Loses consciousness (even if brief)
Behaves abnormally
Management of mild head injury
For a mild head injury, no specific treatment may be needed.
However, closely watch the person for any concerning symptoms over the next 24 hours. The signs of a serious head injury can be delayed. While the person is sleeping, wake him or her every 2 to 3 hours and ask simple questions to check alertness, such as "What is your name?"
Bed rest, fluids, and a mild pain reliever such as paracetamol may be prescribed.
Ice may be applied to the scalp, immediately after the trauma, for pain relief and to decrease swelling. Do not apply ice directly to the skin; wrap the ice in a light cloth before applying. Ice should be applied for 20-30 minutes at a time and can be repeated about every 2-4 hours as needed. There is little benefit after 24 hours.
If a child begins to play or run immediately after getting a bump on the head, serious injury is unlikely. However, as with anyone with a head injury, closely watch the child for 24 hours after the incident.
Pain medicine (like paracetamol or ibuprofen) may be used for a mild headache. DO NOT give aspirin, because it can increase the risk of bleeding.
Management of moderate to severe head injury
People with serious closed head injuries are almost always admitted to the hospital for observation and repeated studies to assure that the condition does not worsen. For a moderate to severe head injury, take the following steps:
· Check the person's airway, breathing, and circulation. If necessary, begin rescue breathing and CPR.
· If the person's breathing and heart rate are normal but the person is unconscious, treat as if there is a spinal injury. Stabilize the head and neck by placing your hands on both sides of the person's head, keeping the head in line with the spine and preventing movement. Wait for a doctor’s help.
· Stop any bleeding by firmly pressing a clean cloth on the wound. If the injury is serious, be careful not to move the person's head. If blood soaks through the cloth, DO NOT remove it. Place another cloth over the first one.
· If you suspect a skull fracture, DO NOT apply direct pressure to the bleeding site, and DO NOT remove any debris from the wound. Cover the wound with sterile gauze dressing.
· If the person is vomiting, roll the head, neck, and body as one unit to prevent choking. This still protects the spine, which you must always assume is injured in the case of a head injury. (Children often vomit ONCE after a head injury. This may not be a problem, but call a doctor for further guidance.)
· Apply ice packs to swollen areas.
· Medication to prevent seizures may be given to prevent or treat seizures that occur from the head injury. Seizures after head injury often do not require treatment because they may not reoccur.
· Penetrating head injuries often require some sort of surgery, usually to remove foreign material or to stop bleeding. Other options include pressure monitors, medication to prevent seizures, and antibiotics to prevent infection. People with this type of injury may need a breathing tube inserted to help prevent further brain injury. Angiography may be performed.
DO NOT
DO NOT wash a head wound that is deep or bleeding a lot
DO NOT remove any object sticking out of a wound
DO NOT move the person unless absolutely necessary
DO NOT shake the person if he or she seems dazed
DO NOT remove a helmet if you suspect a serious head injury
DO NOT pick up a fallen child with any sign of head injury.
Prevention
Make sure you advise the general public about the following:
Wear helmets when bike riding, driving motorcycles, and other similar activities.
Always use safety equipment during activities that could result in head injury. These include car seat belts and hard hats.
Obey traffic signals when riding a bicycle. Be predictable so that other drivers will be able to determine your course.
Be visible. DO NOT ride a bicycle without a light at night.
Use age-appropriate car seats.
Make sure that children have a safe area in which to play.
Supervise children of any age.
Lesson 4: Practical
Role play 1
The role play involves two students:
§ One student is to play the role of a dispenser who is attending a patient with a mild head injury and provide management to the patient.
§ The other student is to play the role of the patient.
Role play 2
The role play involves two students:
§ One student is to play the role of a dispenser who is attending a patient with moderate to severe head injury and provide management to the patient.
§ The other student is to play the role of the patient.
Role play 3
The role play involves two students:
§ One student is to play the role of a dispenser who is attending a man who has come to get some medicines for his small daughter. You notice that the man and his daughter came on a motorbike but are not wearing helmets.
§ The other student is to play the role of the man with the small daughter.
§ Discuss with the man what he can do to prevent head injuries.
Lesson 5: Spinal cord injury:
First aid
Spinal cord injury (SCI) is always a medical emergency as it could lead to chronic painful conditions, permanent paralysis or even death.
SCI occurs when a traumatic event (usually a car, diving or sport accident) results in damage to cells within the spinal cord or severs the nerve tracts that relay signals up and down the spinal cord. The most common types of SCI include contusion (bruising of the spinal cord) and compression (caused by pressure on the spinal cord). Other types of injuries include lacerations (severing or tearing of some nerve fibers, such as damage caused by a gun shot wound), and central cord syndrome (specific damage to the corticospinal tracts of the neck region of the spinal cord).
The types of disability associated with SCI vary greatly depending on the severity of the injury, the segment of the spinal cord at which the injury occurs, and which nerve fibers are damaged. Usually the higher up in the cervical spine the injury, the greater the damage.
If treated correctly, most people with SCI regain some functions between a week and six months after injury, but the likelihood of spontaneous recovery diminishes after six months. Rehabilitation strategies can minimize long-term disability.
Signs
Person is lying with his head, neck or back in an awkward position
Severe pain in the head, neck or back
Weakness, tingling or loss of sensation below the point of injury,
Inability to move arms or legs
Bruises on the head, neck, shoulders or back
Loss of bowel or bladder control
Difficulty breathing
Unconsciousness
Symptoms of shock
Even if the person does not have any of these symptoms but you know he has sustained a back, neck or head injury, treat it as a spinal injury. If a head injury was sustained and the person has disturbed level of consciousness, suspect a spinal injury as well.
Get doctors’ help immediately if:
You suspect a spinal injury. The sooner a person is treated in hospital, the greater the chances for recovery.
First Aid Treatment:
If you suspect a spinal injury, DO NOT move the person unless there is imminent danger from, for example, traffic or fire or you need to perform CPR.
If the person is in the water, don't move him or her to land. Keep the person lying face up until help arrives. The water will immobilize the spine.
Don't remove helmets unless you need to perform CPR.
If the person must be moved, then there should be one person controlling the neck and head to keep them in alignment, and at least two people on either side of the person to lift the person without moving the spine.
Treat other life-threatening injuries while waiting for help to arrive.
Keep the person warm.
Don't give anything to eat or drink.
Lesson 6: Stroke
Signs of a stroke
These include:
weakness, paralysis (inability to move) or numbness of the face or limbs, particularly on one side of the body;
vision suddenly becoming blurred or decreased, especially in one eye;
difficulty talking or understanding speech;
sudden difficulty swallowing;
an unexplained fall, dizziness or loss of balance — someone suffering from stroke may resemble a drunk person;
sudden severe headache with no known cause; and
drowsiness, confusion or loss of consciousness.
What to do if stroke is suspected?
Follow the DRABC Action Plan
Follow the ‘DRABC Action Plan’ in every emergency. It helps you determine whether someone has a life-threatening condition and what first aid is needed.
The following plan assumes you will be calling a doctor or referring the patient to the doctor after giving immediate help.
D — check for DANGER (Safety First)
To you.
To others.
To the affected person.
R — check for RESPONSE
Ask the patient his/her name. Stroke patients may not be able to talk, so grasp both hands and ask them to squeeze — they may respond by squeezing one of your hands.
Does the patient respond? If so, he or she is conscious. Follow the plan at Section II below.
SECTION I
If the person does not respond, he or she is probably unconscious. Make sure you call a doctor or an ambulance for referring the patient to a doctor.
A — check AIRWAY
Is the airway clear of objects?
Is the airway open?
If the airway is not clear, turn the person into recovery position Figure 12.
Kneel beside the person.
Put patient’s arm that is farthest from you out at right angles to patient’s body.
Place patient’s nearer arm across patient’s chest.
Bend patient’s nearer leg up at the knee; the other leg should be straight.
While supporting patient’s head and neck, roll the patient away from you.
When the patient is on the side, keep the top leg bent at the knee, with the knee touching the ground.
Figure 12
Then tilt the head slightly backwards and downwards to let anything that’s in the airway (such as vomit) drain out, and clear the airway with your fingers.
B — check for BREATHING
Tilt the head back.
Is the patient’s chest rising and falling?
Can you hear the patient’s breathing?
Can you feel the breath on your cheek?
If the person is not breathing:
turn the patient onto the back;
tilt the head backwards;
lift the chin, pinch the nose closed and give 2 initial mouth-to-mouth breaths;
make sure the chest rises and falls with each breath; and
if breathing does not return and there are no signs of life, go to the next step (step C).
If the patient is breathing, follow steps below under ‘while waiting for doctor’.
C — give CPR
Kneeling beside the patient, give 30 chest compressions on the lower half of the breastbone. Use 2 hands with the fingers interlocked.
Then tilt the head backwards, tilt the chin and give 2 mouth-to-mouth breaths while pinching the nose shut.
Keep alternating between 30 compressions and 2 breaths until the patient shows signs of life or doctor arrives.
SECTION II
While waiting for doctor, If the patient is conscious:
lie the patient down with the head and shoulders raised and supported (use pillows or cushions);
keep them at a comfortable temperature;
loosen any tight clothing;
wipe away any secretions from the mouth;
make sure the airway is clear and open;
assure the patient that help is on the way (they may be able to communicate by squeezing your hands if they can’t speak) and;
do not give them anything to eat or drink.
If the affected patient becomes unconscious, put them in the recovery position as described above to prevent anything (blood, saliva, or their tongue) from blocking the windpipe and choking them. Continue to monitor the airway and breathing, and be ready to resume the DRABC plan as necessary.
Even if the symptoms are short-lived — a ‘mini-stroke’ or transient ischemic attack (TIA) — ensure the patient is seen by a doctor immediately, as these symptoms can be a warning sign of a future stroke.
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: Human body
Sub-unit 2.5 Date: ________________________
The central nervous system comprises (circle the 2 correct answers)
a. Cranial nerves
b. Brain
c. Spinal cord
d. Spinal nerves
The peripheral nervous system is the larger part of the nervous system
True False
The spinal cord is the continuation of the brain
True False
The spinal cord and brain are covered by meninges
True False
Cranial nerves have the following number of pairs (circle the 1 correct answer)
a. 31
b. 12
c. 13
d. 21
Spinal nerves have the following number of pairs (circle the 1 correct answer)
a. 31
b. 12
c. 13
d. 21
The autonomic nervous system is subdivided into (circle the 2 correct answers)
a. Sympathetic nervous system
b. Sensory-somatic nervous system
c. Cranial nerves
d. Parasympathetic nervous system
Following are the actions of the sympathetic nervous system (circle the 2 correct answers)
a. Increased blood flow of the gastrointestinal tract causing increased digestion
b. Constriction of the pupil and lens
c. Dilatation of the pupils
d. Decreased digestion
The signs of a serious head injury can be delayed
True False
Ice may be applied to the scalp for pain relief and to decrease swelling
True False
Ice should be applied directly to the skin
True False
Mention any five signs suggesting a serious head injury
a. ____________________________________________
b. ____________________________________________
c. ____________________________________________
d. ____________________________________________
e. ____________________________________________
Mention four common causes of head injury
a. ____________________________________________
b. ____________________________________________
c. ____________________________________________
d. ____________________________________________
Notes
Sub-unit 2.6
The Excretory System
Learning objectives:
After completing sub-unit 2.6 dispenser students will be able to:
a. describe routes of excretion of wastes products from human body
b. name major parts of the excretory system and mark their position on human body
c. describe functions of major parts of the excretory system
d. identify common diseases affecting the urinary system.
Introduction
The excretory system is the system that performs the function of excretion, the process of discharging wastes from the body. There are several parts of the body that are responsible for this process, such as the sweat glands, the liver, the lungs, and the kidneys. The kidneys, however, are the major excretory organs and are part of the urinary system (the focus of this chapter). Every day, the kidneys filter nearly 180 to 200 liters of fluid from the blood, allowing waste products to leave the body in urine while returning needed substances to the blood. The rate of filtration is approximately 125 ml/min or 45 gallons (180 liters) each day. Considering that you have 7 to 8 liters of blood in your body, this means that your entire blood volume gets filtered approximately 20 to 25 times each day!
Lesson 1: Anatomy of the Urinary System
The urinary system includes two kidneys, two ureters, the bladder, and the urethra.
Kidneys
The two kidneys are located in the middle of the back part of the abdomen one on each side of the vertebral column. The right kidney usually is slightly lower than the left because the liver displaces it downward. Above each kidney is an adrenal gland (see Unit 2, Sub-unit 2.8, endocrine organs). In a normal adult, each kidney is about 10 cm long, 5.5 cm wide and about 3 cm thick, weighing 150 grams. It is roughly bean-shaped.
Each kidney is surrounded by a thick layer of fat, which helps to protect it. A tough renal capsule closely covers each kidney and provides support for the soft tissue that is inside.
The outer portion of the kidney is called the renal cortex, which lies directly beneath the kidney's covering. Deep to the cortex lies the renal medulla.
The basic structural and functional unit of the kidney is the tiny nephron which is the blood-processing unit, carrying out the formation of urine. There are more than a million nephrons within each kidney.
Urinary bladder
The urinary bladder is a hollow, muscular, and distensible organ shaped like a balloon that lies in the pelvic cavity. The bladder stores urine excreted by the kidneys; it swells into a round shape when it is full and gets smaller when empty. Urine enters the bladder via the two ureters and exits to the outside via the urethra. The urinary bladder usually holds 400–620 mL of urine, but it can hold twice this amount without rupturing if, for example, the outflow is obstructed.
The bladder has a muscular layer; when the bladder is stretched due to the urine, this signals the parasympathetic nervous system (see Unit 2, Sub-unit 2.5, Nervous System) on to contract the muscle which increases pressure on the bladder and creates urinary flow. This makes the bladder to expel urine through the urethra. Circular muscles called sphincters regulate the flow of urine from the bladder. Problems with these muscles can lead to incontinence of urine.
Ureters
The two ureters are the ducts that carry urine from the kidneys to the urinary bladder. The ureters are muscular tubes that move urine along by the motions of peristalsis (just as in the digestive system). In the adult, the ureters are usually 25-30cm long and have a diameter of about 3 millimeters.
The ureters enter the bladder through its back, running within the wall of the bladder for a few centimeters. The backflow of urine is prevented by valves, pressure from the filling of the bladder, and the tone of the muscle in the bladder wall.
Urethra
The urethra is a tube which connects the urinary bladder to the outside of the body. The urethra has an excretory function to pass urine to the outside in both males and females, and also a reproductive function in the male, as a passage for semen. The external urethral sphincter is a muscle that allows voluntary control over urination.
In males, the urethra is about 20 cm long and opens at the end of the penis. In females, the urethra is only about 3-5 cm long and opens externally besides the vaginal opening.
Figure 1: Urinary system (front view)
Figure 2: Urinary system
Figure 3: Urinary system
Figure 4
Activity
Have a look at Figures 5 and 6. With the help of a chalk, mark the position of kidneys, ureters and urinary bladder on your friend’s body.
Figure 5: Location of kidneys in the body (back of the body)
Figure 6: Location of kidneys, ureters and bladder in the body (front of the body)
Lesson 2: Physiology of the urinary system
The kidneys are the primary organs of the urinary system. The kidneys are the organs that filter the blood, remove the wastes, and excrete the wastes in the urine. The waste products in the blood come from the normal breakdown of body tissues and from the food we eat. After the body has taken what it needs from the food (protein, electrolytes, chemicals etc), waste is sent into the blood to be removed by the urinary system. If the kidneys did not remove these wastes, the wastes would build up in the blood and damage the body and may even cause death.
The other components of the urinary system are accessory structures to eliminate the urine from the body.
Kidney nephrons make urine in the following way:
§ Blood is filtered
§ The necessary fluid and chemicals like sodium, phosphorus, and potassium are reabsorbed into the blood and are returned to the body under the influence of local and systemic hormones (see Unit 2, sub-unit 2.8, Endocrine System)
§ The waste products are secreted in the urine.
Humans produce about 1.5 liters of urine over 24 hours, although this amount may vary according to circumstances. For example, in cold weather more urine is produced and when a person is fasting less urine is produced.
Activity
§ Why is more urine produced during cold weather?
§ Why does a person produce less urine when fasting?
§ What are some of the other situations where less urine is produced?
Urination is a conscious process, initiated by stretch receptors in the bladder wall which signal to the brain that the bladder is full. The desire to urinate usually starts when the bladder reaches around 75% of its working volume. This is felt as an urge to urinate. If the person is distracted the desire can fade and return with more urgency as the bladder continues to fill. When urination is initiated, the sphincter relaxes and the muscle contracts, producing urinary flow.
Activity
If the urinary bladder can usually hold 400–620 ml of urine, what will be its volume when the desire to urinate will be felt?
Figure 7
Just concentrate on the right half of Figure 7 to understand the major function of kidneys, i.e. cleaning blood from waste products.
Lesson 3: Disease states
Renal function is said to be 100 % in a person with two healthy kidneys. This is more renal function than a person actually needs. Even people born with only one kidney or people who donate a kidney for transplantation are able to lead normal, healthy lives. Thus, small declines in kidney function may not cause a problem.
A person has serious health problems if they have less than 25 % of their kidney function. If the function drops below 10 - 15 %, the person cannot live long without some form of kidney replacement therapy—either dialysis or transplantation.
Signs and symptoms of kidney disease
Early stages: people do not feel sick
Advanced stages
§ Too much or too little urination
§ Tiredness
§ Itchiness
§ Loss of appetite, nausea and vomiting
§ Swelling or numbness of hands or feet
§ Drowsiness or trouble concentrating
§ Muscle cramps
Presence of protein in urine
Diseased kidneys may fail to separate a blood protein called albumin from the wastes. At first, only small amounts of albumin may leak into the urine, a condition known as microalbuminuria. This is a sign of deteriorating kidney function. As kidney function worsens, the amount of albumin and other proteins in the urine increases, and the condition is called proteinuria. Doctors test for protein using a dipstick in a small sample of urine. The color of the dipstick indicates the presence or absence of proteinuria.
Diabetic Nephropathy
In diabetes, blood levels of glucose are abnormally high. Damage to the nephrons from excess glucose in the blood leads to diabetic nephropathy. If blood glucose levels are kept down, onset of diabetic nephropathy could be prevented or delayed. In diabetes, the target blood pressure should be below 130/80 mmHg or below 125/75 mmHg in people with kidney disease otherwise kidneys may get damaged leading to diabetic nephropathy.1
National Evidence Based Guidelines for the Management of Type 2 Diabetes Mellitus. 2001. NHMRC, Australia.
High Blood Pressure
High blood pressure can damage the small blood vessels in the kidneys. The damaged vessels cannot filter wastes from the blood as they are supposed to.
Acute Renal Failure
Some kidney problems happen quickly, like an accident that injures the kidneys. Losing a lot of blood can cause sudden kidney failure. Some drugs or poisons can make the kidneys stop working. These sudden drops in kidney function are called acute renal failure (ARF). ARF may lead to permanent loss of kidney function. But if the kidneys are not seriously damaged, acute renal failure may be reversed.
Chronic Kidney Disease
Most kidney problems happen slowly. A person may have “silent” kidney disease for years. Gradual loss of kidney function is called chronic kidney disease (CKD). People with CKD may go on to permanent kidney failure. They also have a high risk of dying from a stroke or heart attack.
End-Stage Renal Disease
Total or nearly total and permanent kidney failure is called end-stage renal disease (ESRD). People with ESRD must undergo dialysis or transplantation to stay alive.
Urinary incontinence
It is involuntary urination beyond the age of anticipated control. Inability to hold urine in the urinary bladder is due to loss of voluntary control over the urinary sphincters, is often temporary, and almost always results from an underlying medical condition.
Infections
Cystitis is inflammation of the urinary bladder. Cystitis occurs when the normally sterile lower urinary tract (urethra and bladder) is infected by bacteria and becomes inflamed. The condition more often affects women because of their short length of the urethra, but can affect both males and females and all age groups.
Symptoms of cystitis
· Pressure in the lower pelvis
· Painful urination (dysuria)
· Frequent or urgent need to urinate
· Need to urinate at night
· Cloudy urine
· Blood in the urine (hematuria)
· Foul or strong urine smell
Urethritis
It is inflammation of the urethra. It is a common cause of painful and frequent urination. In men, there may be a discharge which could be purulent or clear. In women discharge may not be present.
Catheterisation
A urinary catheter is any tube system placed in the body to drain and collect urine from the bladder.
Indications for catheterization
§ Acute or chronic urinary retention
§ Orthopedic procedures that may limit a patient's movement
§ Need for accurate monitoring of input and output (such as in an ICU)
§ Benign prostate enlargement
§ Incontinence
§ Patients undergoing surgery
Long term (indwelling) urethral catheters
A catheter that is left in place for a period of time may be attached to a drainage bag to collect the urine. There are 2 types of drainage bags:
a. Leg bag, which is a smaller drainage device that attaches by elastic bands to the leg. A leg bag is usually worn during the day since it fits discreetly under clothes, and is easily emptied into the toilet.
b. A larger drainage device (down drain) that may be used during the night. This device is usually hung on the bed or placed on the floor.
Long-term catheterization can expose patients to an increased risk of infection. During long-term use, the catheter may be left in place during the entire time, or a patient may be instructed on a procedure for placing a catheter just long enough to empty the urinary bladder and then removing it (known as intermittent self-catheterization).
Short-term catheterisation
In some situations, incontinent patients are catheterized. A condom catheter, which fits on the outside of the penis using adhesive, can be used for short-term catheterisation in males.
Complications of catheter use
§ Urinary tract or kidney infections
§ Blood infections (septicemia)
§ Urethral injury
§ Skin breakdown
§ Urinary bladder stones
§ Blood in the urine (hematuria)
§ Urinary bladder cancer (after many years of catheter use)
Lesson 4: Practical
Identify the various types of catheters.
Catheters are available in basically two different styles:
Straight catheter: The straight catheter is a straight tube of pliable plastic or rubber. One end is rounded to prevent any trauma to tissue, with the opening of the lumen (the opening) down the center of the tube on the side. The other end of a catheter is enlarged to form a connection to some type drainage or collection system, and more importantly prevent the catheter from being completely "lost" into the urethra.
Figures 8: Straight catheter
Figure 9
Foley catheter: Foley catheter is designed for in-dwelling, long-term use. The catheter has two lumens extending its length, essentially two tubes in one, one ending in an opening near the end for draining the bladder, the other communicating with a balloon just below the drainage opening which can be inflated with sterile water once it is inside the bladder anchoring it in place and preventing it from slipping back out until the balloon is deflated. NEVER use air for inflating in the bladder. The drainage lumen terminates in the same type of connector as the straight catheter, and the balloon lumen terminates in a valve arrangement which allows the balloon to be inflated with sterile water and deflated.
Catheters come in a large variety of sizes and materials (latex, silicone, PVC, or Teflon). If people develop allergies or sensitivity to latex after long-term latex catheter use, they should use the other types of catheters.
In the case of internal catheters, those inserted into the urethra, the smallest size is usually recommended, although a larger size is sometimes needed to control leakage of urine around the catheter. A large size can also become necessary when the urine is thick, bloody or contains large amounts of sediment. Larger internal catheters, however, are more likely to cause damage to the urethra.
Figures 10: Foley catheter
Figure 11
Insertion of a catheter (men)
i. Assemble all equipment: catheter, lubricant, sterile gloves, cleaning supplies, syringe with water to inflate the balloon, drainage receptacle.
ii. Wash your hands. Use betadine or similar cleansing product (unless instructed otherwise) to clean the urethral opening.
iii. Apply the sterile gloves. Make sure you do not touch the outside of the gloves with your hands.
iv. Lubricate the catheter.
v. Hold the penis on the sides, perpendicular to the body. Stretch the penis away from the body.
vi. Begin to gently insert and advance the catheter.
vii. You will meet resistance when you reach the level of the external sphincter. Try to relax by deep breathing, and continue to advance the catheter.
viii. Once the urine flow starts, continue to advance the catheter to the level of the "Y" connector. Hold the catheter in place while you inflate the balloon. Some men have developed urethral injuries due to the balloon being inflated in the urethra and not in the urinary bladder. Care must be taken to ensure the catheter is in the urinary bladder. You may try to irrigate the catheter with a few milliliters of sterile water. If the solution does not easily return, you may not have the catheter far enough in the bladder.
ix. Secure the catheter, and attach the drainage bag.
Insertion of a catheter (women)
i. Assemble all equipment: catheter, lubricant, sterile gloves, cleaning supplies, syringe with water to inflate the balloon, drainage receptacle.
ii. Wash your hands. Use betadine or cleansing product to clean the urethral opening. In women clean the external genitalia and urethral meatus (opening which is located below the clitoris and above the vagina) using downward strokes. Avoid the anal area.
iii. Apply the sterile gloves. Make sure you do not touch the outside of the gloves with your hands.
iv. Lubricate the catheter.
v. Spread the genital lips and locate the meatus.
vi. Slowly insert the catheter into the meatus.
vii. Begin to gently insert and advance the catheter.
viii. Once the urine flow starts, advance the catheter another 2 inches. Hold the catheter in place while you inflate the balloon. Care must be taken to ensure the catheter is in the urinary bladder. If pain is felt while inflating the balloon, stop. Deflate the balloon; advance the catheter another 2 inches, and attempt to inflate the balloon again.
ix. Secure the catheter, and attach the drainage bag.
OR the following
Insertion of a Straight catheter
The penis is first pulled up to a right angle to the body or even slightly higher. This straightens out the first half of the normal "S" curve to the urethra, as shown in the illustration. The catheter and the opening of the penis should be well lubricated with a sterile water-soluble lubricant such as KY from a freshly opened tube. If at all possible, the three or more inches of the catheter closest to the tip should remain "untouched by human hands."
Figure 12
The catheter is guided gently into the opening in the end of the penis. It should go fairly easily for the first six to twelve inches, and then it is normal to encounter some resistance. You will also, probably at the same time as you encounter resistance, perceive a change in the reaction of the person receiving the catheter. This means that the tip of the catheter is now in the area of the prostate, causing an altered sensation in that area, and encountering the sphincter muscles, which are probably closed at this time. A little firm, gentle pressure will usually overcome this resistance, resulting in a flow of urine through the catheter (did you provide something to catch it in?).
Insertion of a Foley catheter
A Foley catheter is inserted using the same technique as described for the straight catheter above; however; the balloon should not be inflated until a urine return has been obtained and the catheter advanced another two to three inches to ensure that the balloon is entirely within the urinary bladder and not in the urethra, where inflation of the balloon could result in serious damage.
Figure 13: Foley catheter in place (top: female; bottom: male)
Figure 14: Foley catheter in place (male)
Activity
The role play involves two students:
§ One student is to play the role of a dispenser who has inserted a catheter into a patient with urinary retention.
§ The other student is to play the role of the patient with the inserted catheter.
§ The two students should discuss the following points related to catheter insertion:
Things you should tell the patient with an inserted catheter
i. Routine changing (replacing) of the catheters should not be done. However, if the catheter is clogged, painful, or infected it may require immediate replacement.
ii. Routine care of the indwelling catheter MUST include daily cleansing of the urethral area (where the catheter exits the body) and the catheter itself with soap and water. The area should also be thoroughly cleansed after passing stools to prevent infection. There is no need to use antimicrobial ointments around the catheter as they have not been shown to reduce infections.
iii. You should increase your fluid intake to reduce the risk of developing complications.
iv. The drainage bag must always stay lower than the urinary bladder to prevent a back flow of urine back up into the urinary bladder. The drainage device should be emptied at least every 8 hours, or when the device is full. Care must be taken to keep the outlet valve from becoming infected. Wash your hands before and after handling the drainage device. Do not allow the outlet valve to touch anything. If the outlet becomes dirty, it should be cleaned with soap and water.
v. Cleaning of the drainage bag: Remove the drainage bag from the catheter (attach the catheter to a second drainage device during the cleansing). Cleanse and deodorize the drainage bag by filling the bag with 2 parts vinegar and 3 parts water. Chlorine bleach can be substituted for the vinegar and water mixture. Let this solution soak for 20 minutes. Hang the bag with the outlet valve open to drain and dry the bag.
vi. Notify your health care provider if you develop any of the following:
§ Urine with a strong smell or urine becomes thick or cloudy
§ Fever, chills
§ Urethral swelling around the catheter
§ Bleeding into or around the catheter
§ Catheter draining little or no urine despite adequate fluid intake
§ Leakage of large amounts of urine around the catheter.
How to remove a catheter
Indwelling catheters may be removed in 2 ways:
(a) Attach a small syringe to the inflation port on the side of the catheter. Draw out all the fluid until you are unable to withdraw any more fluid. Slowly pull the catheter out until it is completely removed.
(b) Cut the inflation port tubing before it reaches the main tubing of the catheter. After all the water has drained out, slowly pull out the catheter until it is completely removed. Be careful not to cut the catheter anywhere else.
If the patient is unable to urinate within 8 hours after catheter removal, or if the abdomen becomes distended and painful, the patient should immediately report to a health care provider.
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: Human body
Sub-unit: 2.6 Date: _________________________
The urinary system is sometimes referred to as the excretory system because one aspect of its function is to rid the body of waste products.
True False
The kidneys are the organs that filter the blood, remove the wastes, and excrete the wastes in the urine.
True False
The following organs are part of the excretory system (circle all the correct answers).
a. Sweat glands
b. Trachea
c. Lungs
d. Brain
Each normal adult kidney has about the following number of nephrons (circle one).
a. One million
b. Two million
c. Three million
Fill in the blanks by choosing the answers from the following list:
§ Liver
§ Neuron
§ Nephron
§ Kidneys
§ Urethra
§ Gall bladder
§ Urinary bladder
§ Ureters
Name the different organs of the urinary system.
a. __________________
b. __________________
c. __________________
d. __________________
The functional unit of the kidney is a ________________.
The ______________ transport urine from the _____________ to the ____________.
Urine is temporarily stored in ___________________.
The _______________ is the final passageway for the flow of urine
Every day, the kidneys filter nearly _____ liters of fluid from the blood.
People with diabetes or reduced kidney function have a target blood pressure below _________ mm Hg.
Label the following diagram 1 of the urinary system.
Diagram 1
Notes
Sub-unit 2.7
Reproductive System
Learning objectives:
After completing sub-unit 2.7 dispenser students will be able to:
a. identify major parts of the reproductive system
b. describe functions of major parts of the reproductive system
c. identify common disease condition affecting the reproductive system
d. give health promotion messages related to reproductive health.
1. Lesson 1: Anatomy of the reproductive system
Male reproductive system
The reproductive organs of the male can be grouped into three categories:
i. Organs for sperm production and storage: sperm are produced in the testes which are located in the temperature-regulating scrotum; immature sperm then travel to the epididymis for further development and storage
ii. Glands which produce the sperm-containing fluid called semen: these include the seminal vesicles, prostate, and the vas deferens
iii. Organs used for mating and deposition of the spermatozoa within the female: these include the penis, urethra, vas deferens, and Cowper's gland.
Testes are oval-shaped and grow to be about 5 cm in length and 3 cm in diameter.
The epididymis is a long coiled tube on the testes where sperms are stored. It connects to the vas deferens.
The vas deferens is a muscular tube that passes upward alongside the testes and transports the sperm-containing fluid called semen. It connects epididymis with the urethra.
The seminal vesicles are sac-like structures attached to the back of the urinary bladder. The duct of each seminal vesicle joins the duct of the vas deferens on the same side to form the ejaculatory duct. Their secretions provide the bulk of the semen.
The prostate gland, lies below the urinary bladder. It produces part of the semen.
The urethra is the tube that carries the sperms and semen to the outside of the body through the penis. The urethra is also part of the urinary system because it is also the channel through which urine exits the body (see Unit 2, Sub-unit 2.6, Urinary System).
The scrotum is a pocket-like structure of skin behind the penis in which the epididymis and the testicles hang. This bag helps to regulate the temperature of testes, which need to be kept cooler than body temperature to produce sperm.
The penis is made up of two parts: the shaft and the glans. The shaft is the main part of the penis and the glans is the tip. At the end of the glans is a small opening, which is where semen and urine exit the body through the urethra. The inside of the penis is made of a spongy tissue that can expand and contract.
Figure 1: Male reproductive organs
Figure 2: Male reproductive organs
Female reproductive system
The internal reproductive organs of the female are the:
ovaries, which produce the ova (eggs)
two fallopian tubes, which connect the ovaries with the uterus
uterus, which holds the developing fetus, and
vagina, which opens outside and acts as the container for the male's sperm.
The external part of the female reproductive organs is called the vulva. Located between the legs, the vulva covers the opening to the vagina and other reproductive organs located inside the body.
The ovaries are the main reproductive organs of a woman. The two ovaries, which are about the size and shape of almonds, produce ova (eggs). The ovaries are also part of the endocrine system because they produce female sex hormones such as estrogen and progesterone. All the other female reproductive organs are there to transport, nurture and otherwise meet the needs of the egg or developing fetus.
The fallopian tubes are about 10 cm long. They are two very narrow tubes that lead from the right and the left ovaries into the uterus. They have a number of finger-like projections on the end near the ovary. When an egg is released by the ovary it is ‘caught’ by one of the fingers of the fallopian tubes and transported along the tube into the uterus. It takes the egg about 5 days to reach the uterus and it is on this journey down the fallopian tube that fertilization may occur if a sperm penetrates and fuses with the egg.
The uterus is a hollow cavity shaped like an upside-down pear, with a thick lining called endometrium and muscular walls called myometrium. If an egg has been fertilized, it will burrow into the endometrium, where it will form the fetus. A part of the wall of the fertilized egg, which has burrowed into the endometrium, develops into the placenta. If an egg has not been fertilized, the endometrial lining is shed at the end of each menstrual cycle.
The uterus contains some of the strongest muscles in the female body. These muscles are able to expand to accommodate a growing fetus and then contract to help push the baby out through the vagina during labor.
When a woman is not pregnant, the uterus is only about 7.5 centimeters long and 5 centimeters wide. The uterus has three parts:
Body of the uterus: this is the main part of the uterus
Fundus of the uterus: the rounded region above the entrance of the fallopian tubes
Cervix: the narrow outlet, which protrudes into the vagina.
The vagina is a tube that extends from the cervix to the outside. The vagina receives the penis and semen during sexual intercourse and also provides a passageway for menstrual blood flow to leave the body.
Figure 3: Female reproductive organs
Figure 4
Figure 5: Female reproductive organs
Lesson 2: Physiology of the male and female reproductive systems
Males
The main function of the male reproductive system is to provide the male sex cells called spermatozoa (sperm) for fertilization of the female ovum (egg). In a man who has reached sexual maturity, the two testes, produce and store millions of tiny sperms.
The testes are also part of the endocrine system (see Unit 2, Sub-unit 2.8, Endocrine System) because they produce hormones, including testosterone. Testosterone is primarily secreted in the testes of males and the ovaries of females, although small amounts are also secreted by the adrenal glands. It is the principal male sex hormone.
In both men and women, testosterone plays a key role in health and well-being as well as in sexual functioning. Examples include enhanced sex drive, increased energy, increased production of red blood cells and protection against osteoporosis (bone thinning). On average, an adult human male body produces about forty to sixty times more testosterone than an adult female body, but females are more sensitive to the hormone.
Testosterone is a major part of puberty in boys, and as a boy progresses through puberty, his testes produce more and more of it. Testosterone functions are:
Anabolic effects which include growth of muscle mass and strength, increased bone density and strength, and stimulation of linear growth and bone maturation.
Virilizing effects which include maturation of the sex organs, particularly the penis and the formation of the scrotum in unborn children, and after birth (usually at puberty), a deepening of the voice, growth of the beard and body hair, development of an Adam's apple. Many of these fall into the category of male secondary sex characteristics.
Females
The ovary contains ovarian follicles, in which eggs develop. At certain intervals, typically approximately every 28 days, one follicle from either the right or the left ovary matures and ruptures, and the ovary releases an egg, which passes through the fallopian tube into the uterus. This process is called ovulation which occurs in the middle of the menstrual cycle. If fertilization between a male sperm cell and female egg does not take place, the lining of the uterus, called the endometrium, and unfertilized egg are shed each month through a process known as menstruation.
In females the important sexual hormones include estrogen and progesterone. Estrogen is produced primarily by ovaries and, during pregnancy, in the placenta. While estrogens are present in both men and women, they are usually present at significantly higher levels in women of reproductive age. Estrogen is responsible for the development of the major secondary sexual characteristics which include: a smaller stature than men, a high percentage of body fat, wider hips, reduced muscle mass, development of breast glands, and enlarged breasts.
Progesterone is produced in the adrenal glands, the gonads (ovaries and testes), the brain, and, during pregnancy, in the placenta. Progesterone is sometimes called the "hormone of pregnancy", as it has many roles relating to pregnancy, e.g. progesterone is responsible for the implantation of the fertilized ovum into the uterus.
Puberty
Puberty refers to the process of physical changes by which a child's body becomes an adult body capable of reproduction. Puberty is initiated by hormone signals from the brain to the gonads (the ovaries and testes). In response, the gonads produce a variety of hormones that stimulate the growth, function, or transformation of brain, bones, muscle, skin, breasts, and reproductive organs. Growth accelerates in the first half of puberty and stops at the completion of puberty. Before puberty, body differences between boys and girls are almost entirely restricted to the genitalia. During puberty, major differences of size, shape, composition, and function develop in many body structures and systems. The most obvious of these are referred to as secondary sex characteristics (see above).
Two of the most significant differences between puberty in girls and puberty in boys are the age at which it begins, and the major sex hormones involved. Although there is a wide range of normal ages, on average, girls begin the process of puberty about 1-2 years earlier than boys (with average ages of 9-14 years for girls and 10-17 years for boys), and reach completion in a shorter time. Girls attain adult height and reproductive maturity about 4 years after the first physical changes of puberty appear. In contrast, boys accelerate more slowly but continue to grow for about 6 years after the first visible pubertal changes.
The hormone that dominates female development is estrogen. In males, testosterone is the principal sex steroid. The male growth spurt also begins later, accelerates more slowly, and lasts longer before the long bones stop growing. Although boys are 2 cm shorter than girls before puberty begins, adult men are on average about 13 cm (5.2 inches) taller than women.
Menopause
Menopause means the natural and permanent stopping of the monthly female reproductive cycles, and in humans this is usually indicated by a permanent absence of monthly periods or menstruation. However, if for medical reasons, the uterus is surgically removed in a younger woman, and after this her monthly periods cease permanently, the woman will technically be infertile, but as long as at least one of her ovaries still functions, the woman will not have entered menopause. This is because even without the uterus, ovulation, and the release of the reproductive hormones that are an essential part of the reproductive cycles, will continue until the time of menopause is reached.
The average age of menopause is 51 years. The normal age range for the occurrence of menopause is somewhere between the age of 45 and 55. Menopause is triggered by the decreasing function or surgical removal of the ovaries. Menopause starts as the ovaries begin to fail to be able to produce an egg every month. Since the process of producing and ripening the egg is also what creates several of the key hormones involved in the monthly cycle, this in turn interrupts the regular pattern of the hormone cycles, and gradually leads to the shutting down of the whole reproductive system.
The break-up in the pattern of the menstrual cycles not only causes the levels of most of the reproductive hormones to drop over time, but also causes the reproductive hormones to fall out of phase with one another, which often leads to extreme and unpredictable fluctuations in the levels, which itself can cause numerous symptoms in most women, such as hot flashes.
After a number of years of abnormal functioning, the ovaries almost completely stop producing the estrogen hormones and progesterone but testosterone levels do not drop significantly during the menopause transition; the postmenopausal ovary and the adrenal gland still continue to secrete a reasonable amount of testosterone in post-menopause, at least in most women. Because of the various hormonal changes, the reproductive system ceases to function.
Menopause symptoms
· Lack of energy
· Hot flashes, night sweats and palpitations
· Depression, anxiety, irritability, mood swings and lack of concentration
· Vaginal dryness and urgency of urination.
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: 2.7
Sub-unit 2.7 Date: ________________________
The reproductive organs of the male can be grouped into how many categories? (circle the correct answer)
e. Two
f. Three
g. Four
Sperm are produced in the ___________ which are located in the temperature-regulating ____________.
Sperms are stored in (circle the correct answer).
e. Seminal vesicles
f. Prostate gland
g. Epididymis
Briefly describe the function of ovaries and uterus.
________________________________________________________________________________________________________________________________________________________________________________________________________________________
___________________ are two very narrow tubes that lead from the right and the left ovaries into the ____________.
Testes and ovaries apart from being parts of the reproductive system are also parts of the ____________ system.
Testosterone is produced by
c. __________________
d. __________________
e. __________________
f. __________________
Testosterone is present in both males and females
True False
Estrogen and progesterone are present in both males and females
True False
Virilizing effects of testosterone include the following.
_____________________________________________________________________
_______________________________________________________________________________________________________________________________________________________________________________________________________________
In females, eggs are developed in _____________.
Major secondary sexual characteristics of females include:
_____________________________________________________________________
_______________________________________________________________________________________________________________________________________________________________________________________________________________
Estrogen is sometimes called the "hormone of pregnancy", as it has many roles relating to pregnancy.
True False
Briefly describe puberty.
________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________
Briefly describe menopause.
________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________
Notes
Sub-unit 2.8
The Endocrine System
Learning objectives:
After completing sub-unit 2.8 dispenser students will be able to:
a. name major parts of the endocrine system
b. describe functions of major parts of the endocrine system
c. identify common diseases affecting the endocrine system
d. deliver health promotion and family planning (family welfare) messages related to this system.
Introduction
The endocrine system is a signal system much like the nervous system. The endocrine system, along with the nervous system, functions in the regulation of body activities. The nervous system acts through electrical impulses and neurotransmitters to cause muscle contraction and glandular secretion. The effect of nervous system stimulation is of a short duration, measured in milliseconds, and localised. The endocrine system acts through chemical messengers called hormones which are released into the blood and travel long distances throughout the body. Hormones influence growth, development, and metabolic activities. The action of the endocrine system is measured in minutes, hours, or weeks and is more generalised than the action of the nervous system.
1. Lesson 1: Anatomy of the endocrine system
A gland is an organ that synthesizes a substance for release. Glands can be divided into two groups:
Exocrine glands
These are glands that secrete their products via a duct into cavities inside the body or on its outer surface, e.g. mucus, digestive juices, saliva, sweat.
Endocrine glands
These are glands that secrete their product or chemical messengers called hormones directly into the blood stream. They do not have ducts to carry their product to a surface and are therefore called ductless glands. Endocrine glands have a rich drainage of blood through which hormones circulate throughout the body where they influence only those cells that have receptors for that hormone.
Main endocrine glands
§ Hypothalamus: in the brain
§ Pituitary gland: in the brain
§ Pineal gland: in the brain
§ Thyroid gland: in the neck
§ Parathyroid gland: in the neck
§ Pancreas: in the abdomen
§ Adrenal glands: in the abdomen on top of each kidney
§ Testes and ovaries: in the abdomen
Other organs with some hormone-producing cells
§ Thymus gland
§ Heart
§ Stomach
§ Liver
§ Small intestine
§ Kidney
Figure 1: Location of main endocrine glands
Figure 2: Location of main endocrine glands
Activity
In small groups and consulting Figures 1 and 2 discuss the location of the main endocrine glands in the body.
Lesson 2: Physiology of the endocrine system
Hormones
A hormone is a chemical messenger that carries a signal from one cell to another (secreted by endocrine gland travels through the blood and affects other cells and organs). Hormones are carried by the blood throughout the entire body, yet they affect only certain cells. The specific cells that respond to a given hormone have receptors for that hormone. This is sort of a lock and key mechanism. If the key fits the lock, then the door will open. If a hormone fits the receptor site, then there will be an effect. If a hormone and a receptor site do not match, then there is no reaction. All the cells that have receptor sites for a given hormone make up the target tissue for that hormone. In some cases, the target tissue is localized in a single gland or organ, e.g. thyroid-stimulating hormone (see below) has receptors present only in the thyroid gland. In other cases, the target tissue is diffuse and scattered throughout the body so that many areas are affected, e.g. growth hormone (see below) has receptors present in most organs of the body. Hormones bring about their characteristic effects on target cells by modifying cellular activity.
Hypothalamus, situated in the brain, is the coordinator of the hormonal activity. As shown below, it gets signals from the central nervous system and makes hormones. These hormones act on other endocrine organs which then make their own hormones.
Flow Chart: the hierarchy of the endocrine system
Central nervous system
ê
Hypothalamus
í
ê
î
Anterior pituitary
Posterior pituitary
Kidneys
ê
ê
Thyroid; gonads; skeletal muscles; bones; adrenal glands
Kidneys; gonads
Activity
Ask the students to discuss the hierarchy of the endocrine system with the help of the above Flow Chart. Students draw flow chart to show the hierarchy of the endocrine system.
Although the major endocrine glands are scattered throughout the body, they are still considered to be one system because they have similar functions, similar mechanisms of influence, and many important interrelationships.
Some glands also have non-endocrine regions that have functions other than hormone secretion. For example, the pancreas has a major non-endocrine portion that secretes digestive enzymes (see Unit 2, Sub-unit 2.2, Digestive System) and an endocrine portion that secretes hormones. The ovaries and testes secrete hormones and also produce the ova and sperm (see Unit 2, Sub-unit 2.7, Reproductive System). Some organs, such as the stomach, intestines, and heart, produce hormones, but their primary function is not hormone secretion.
The table below shows the hormones released from the main endocrine glands. Note that the hormones released from the hypothalamus affect the release and inhibition of hormones from the glands placed lower than the hypothalamus.
Table 1 below shows endocrine glands and their secreted hormones
Table 1
Hypothalamus
Secreted hormone
Abbreviation
Effect
Thyrotropin-releasing hormone
TRH
Releases TSH from anterior pituitary
Gonadotropin-releasing hormone
GnRH
Releases FSH and LH from anterior pituitary.
Growth hormone-releasing hormone
GHRH
Releases GH from anterior pituitary
Growth hormone-inhibiting hormone
GHIH
Inhibits release of GH and TSH from anterior pituitary
Corticotropin-releasing hormone
CRH
Releases ACTH from anterior pituitary
Prolactin-releasing hormone
PRH
Releases prolactin from anterior pituitary
Prolactin inhibiting hormone
PIH
Inhibits release of prolactin from anterior pituitary
Vasopressin
Increases water reabsorption from kidneys
Pituitary gland
Secreted hormone
Abbreviation
Effect
Anterior pituitary lobe
Thyroid-stimulating hormone
TSH
Causes thyroid gland to secrete thyroid hormones - thyroxine (T4) and tri-iodothyronine (T3)
Gonadotropic hormones
In females: regulate the development, growth, and function of ovary
In males: regulate the development, growth, and function of testes
Growth hormone
GH
Stimulates growth of bones, skeletal muscles and other organs
Adrenocorticotropic hormone
ACTH
Stimulates synthesis of cortisol in adrenal glands
Prolactin
PRL
Promotes the development of female breast during pregnancy and stimulates milk production after the birth of the baby
Posterior pituitary lobe
Oxytocin
In females: contraction of uterus thus starting childbirth; starts milk ejection from the lactating breast
Antidiuretic hormone
ADH
Stimulates kidneys to reabsorb water, with the result that less water is lost as urine
Pineal Gland
Secreted hormone
Effect
Melatonin
Affects reproductive development and daily physiologic cycles
Thyroid gland
Secreted hormone
Abbreviation
Effect
Tri-iodothyronine
T3
Active form of thyroid hormone: increases the basal metabolic rate
Affects protein synthesis
Thyroxine
T4
Less active form of thyroid hormone: increases the basal metabolic rate
Affects protein synthesis
Calcitonin
Opposes the action of the parathyroid glands by reducing blood calcium levels
Parathyroid gland
Secreted hormone
Effect
Parathyroid hormone
Increases blood calcium levels
Thymus gland
Secreted hormone
Effect
Thymosin
Development of the body's immune (defense) system
Pancreas
Secreted hormone
Effect
Insulin
Decreases blood glucose level
Glucagon
Increases blood glucose level
Adrenal glands
Secreted hormone
Effect
Adrenal cortex
Cortisol
Increases blood glucose levels
Aldosterone
Conserves sodium and water in the body
Androgens and estrogens
Virilization
Adrenal medulla
Adrenaline and Noradrenaline
These two hormones are secreted in response to stimulation by sympathetic nerve, particularly during stressful situations causing fight-or-flight response (see Unit 2, Sub-unit 2.5, Nervous System)
Secreted hormone
Effect
Testes
Testosterone
The growth and development of the male reproductive structures
Increases skeletal and muscular growth
Enlargement of the larynx accompanied by voice changes
Growth and distribution of body hair
Increases male sexual drive
Ovary
Progesterone
Supports pregnancy by causing the uterine lining to thicken in preparation for pregnancy. Together, progesterone and estrogens are responsible for the changes that occur in the uterus during the female menstrual cycle
Estrogens
Development of the breasts
Distribution of fat in the hips, legs, and breast
Maturation of reproductive organs such as the uterus and vagina
Activity
From the list in Table1, discuss examples of three endocrine glands which act on localized target tissue and three endocrine glands which act on diffuse target tissue.
Disease states
Thyroid hormones
Iodine is necessary for the synthesis of the thyroid hormones T3 and T4. If there is an iodine deficiency, the thyroid cannot make sufficient hormone. This stimulates the anterior pituitary to secrete thyroid-stimulating hormone (TSH), which causes the thyroid gland to increase in size in an attempt to produce more hormones. But it cannot produce more hormones because it does not have the necessary raw material, iodine. This type of thyroid enlargement is called simple goiter or iodine deficiency goiter.
According to UNICEF1, 70% of the total population in Pakistan is at risk of iodine deficiency disorders (IDD). Northern areas of Pakistan (Dir, Swat, Chitrral and Gilgit) are highly endemic for IDD2-3. Iodine deficiency is also reported from other parts of the country like Azad Jammu and Kashmir, Peshawar, Swabi, Islamabad, Karachi and Quetta4-9. IDD can only be eliminated by addition of iodine through any mean in the food items e.g. in the table salt.
1. Rafiq M. Prevalence survey of iodine deficiency disorders in 8-10 years old school children and use of iodized salt, Swat District NWFP, Pakistan, 1998.
2. Bano S, Haq MU, Khan SM, Shah SA, Iqbal N. Iodine deficiency still a major health problem in some areas of Swat. Pak J Med Res 1999; 38(1): 3-6.
3. Bano S etal. People still suffer from hidden hunger in Swat, Pakistan. IDD News Letter 1998;1-4:26-7.
4. Zargar AH, Shah JA, Mir MM etal. Prevalence of goitre in school children in Kashmir Valley. Am J Clin Nutr 1995; 62:1020-21.
5. Gardezi SMA. IDD prevalence survey in Azad Jammu and Kashmir. Report 1993. Iodine deficiency disorders in schools of Peshawar. A rapid appraisal survey, Family Health Project. Dept of Health NWFP. Report 1997.
6. Ullah Z, Akhtar T, Khan AU, Nawab G, Haq. Goitre in school children versus use of iodized salt in Peshawar. Pak J Med Res 2001;40(3):90-94.
7. Mohammad S, Ullah Z, Khattak IA, Zai S, Akhtar T. Goitre prevalence and quality of drinking water in district Mardan. Pak J Med Res 1987;27(1):53-56.
8. Carl S. Iodine deficiency disorders in Pakistan, Islamabad, UNICEF1995:p.3.
9. Iqbal N, Haq MU, Khan SM etal. Assessment of iodine deficiency in school going children in Abbottabad-Pakistan. Specialist 1999;15(4):325-329.
Insulin
Activity
Teachers to initiate a class brainstorming session on diabetes to assess what the students know about diabetes.
Insulin is a hormone that is produced by the pancreas and is needed to convert sugar (glucose), starches and other food into energy needed for daily life. When we eat food, the body breaks down all of the sugars and starches into glucose, which is the basic fuel for the cells in the body. Insulin takes the glucose from the blood into the cells. When insulin is absent or deficient, blood sugar levels remain high after a meal because glucose is unable to enter cells. Deficiency or absence of insulin leads to diabetes mellitus which is a metabolic disorder.
There are three types of diabetes mellitus but in this chapter we will only focus on type 2 diabetes which is the most common type of diabetes. In type 2 diabetes, either the:
body does not produce enough insulin, or
cells do not respond to insulin i.e. there is insulin resistance which means that body cells do not respond appropriately even when insulin is present.
People at high risk for type 2 diabetes
§ obese or overweight
§ women who have had diabetes during pregnancy
§ people with family members who have type 2 diabetes
§ people who have a combination of high ‘bad’ fats, low ‘good’ fats and high blood pressure; and
§ older people (however, now type 2 diabetes is increasingly seen in children and adolescents which is due to obesity in this age group)
Type 2 diabetes is often managed by lifestyle modification; it is usually first treated by increasing physical activity and losing weight. These can restore insulin sensitivity even with small weight loss, for example around 5 kg. The usual next step, if necessary, is treatment with antidiabetic drugs by mouth. Such medication may eventually fail due to further decrease of insulin secretion by pancreas. At this point, insulin injections are started.
Symptoms of diabetes
· increased thirst: due to dehydration brain is stimulated to cause a person to drink huge amounts of water
· increased urination: as excessive amounts of glucose are passed out in the urine, it takes along with it huge amounts of water
· increased hunger: although plenty of glucose is available in the blood, it is not available to the body cells and so the person feels hungry all the time
· sudden weight loss
· feeling very tired
Complications of diabetes
Severe long-term complications can result from type 2 diabetes which has either not been diagnosed or not being managed properly:
§ diabetic nephropathy leading to kidney failure
§ vascular disease including coronary artery disease (heart disease) and strokes
§ diabetic retinopathy leading to vision damage and even blindness
§ diabetic neuropathy leading to loss of sensation (heat and cold) or pain
§ diabetic foot complications including ulcers, infections, or gangrene (death of tissue) that may require foot or leg amputation. Foot complications happen when there is nerve damage in the feet and/or when blood flow is reduced (artery disease).
Figure 3: Diabetic foot problems
Figure 4: Diabetic gangrene
Activity
In small groups discuss:
What has happened in the above figures?
Why is it important for diabetics to take good care of their feet?
How can a diabetic stay healthy to avoid complications?
Class room evaluation
Student: _________________________ ID: __________________________
Teacher: _________________________ Unit: Human body
Sub-unit 2.8 Date: ________________________
What are glands and what are their two types?
________________________________________________________________________________________________________________________________________________
What are the characteristics of endocrine glands?
________________________________________________________________________________________________________________________________________________________________________________________________________________________
List the main endocrine glands.
________________________________________________________________________________________________________________________________________________________________________________________________________________________
List the organs in the body that have pockets of hormone-producing cells.
________________________________________________________________________________________________________________________________________________________________________________________________________________________
Draw the human body and indicate where the main endocrine glands are located.
The endocrine gland which is the coordinator of hormonal activity in the body is
____________________________
What are hormones?
________________________________________________________________________
Actions of thyroid hormones include:
________________________________________________________________________________________________________________________________________________________________________________________________________________________
Goitre is an enlarged ______________________ gland.
What is insulin?
a. a hormone that aids in digesting proteins
b. a nutrient that helps filter wastes
c. a hormone that helps to process blood sugar
d. an enzyme that dissolves cholesterol
Where in the body is insulin produced?
a. brain
b. liver
c. pancreas
d. thyroid
Approximately what percent of people with diabetes have type 2 diabetes?
a. 10%
b. 30%
c. 70%
d. 90%
What complications could occur in people with diabetes?
________________________________________________________________________________________________________________________________________________________________________________________________________________________
Notes
{kind=link}
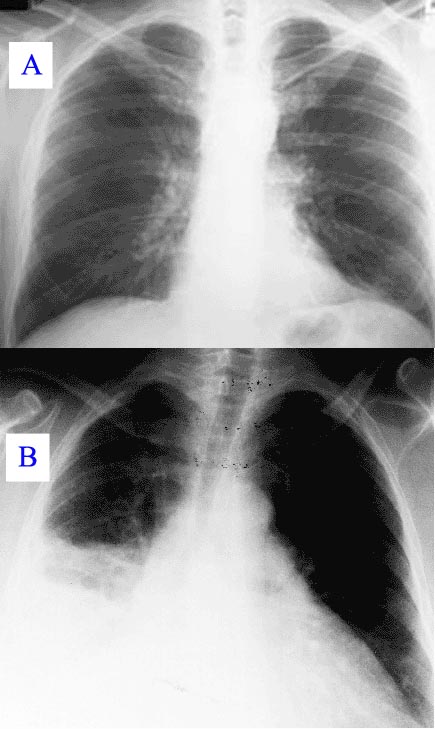{kind=link}
{kind=link}
{kind=link}
{kind=link}
No comments:
Post a Comment